
(PDF format, 1.95 MB, 112 pages)
Organization: Health Canada
Published: 2016-12-13
The Honourable Jody Wilson-Raybould
Minister of Justice and Attorney General of Canada
The Honourable Jane Philpott
Minister of HealthThe Honourable Ralph Goodale
Minister of Public Safety and Emergency Preparedness
Dear Ministers,
Please find attached the final report of the Task Force on Cannabis Legalization and Regulation.
This report is the product of our consultations with Canadians, provincial, territorial and municipal governments, Indigenous governments and representative organizations, youth, patients and experts in relevant fields.
It has been a privilege to consult with so many people over the last five months, and we are deeply thankful to all those who provided their input, time and energy to us.
We hope that this report will be useful to you and your Cabinet colleagues as you move forward with the legalization and regulation of cannabis.
A. Anne McLellan (Chair)
Mark A. Ware (Vice Chair)
Susan Boyd (Member)
George Chow (Member)
Marlene Jesso (Member)
Perry Kendall (Member)
Raf Souccar (Member)
Barbara von Tigerstrom (Member)
Catherine Zahn (Member)
Table of Contents
- Foreword
- Executive Summary
- Chapter 1: Introduction
- Chapter 2: Minimizing Harms of Use
- Chapter 3: Establishing a Safe and Responsible Supply Chain
- Chapter 4: Enforcing Public Safety and Protection
- Chapter 5: Medical Access
- Chapter 6: Implementation
- Annex 1: Biographies of Task Force on Cannabis Legalization and Regulation Members
- Annex 2: Terms of Reference
- Annex 3: Acknowledgements
- Annex 4: Discussion Paper ‘Toward the Legalization, Regulation and Restriction of Access to Marijuana’
- Annex 5: Executive Summary: Analysis of consultation input submitted to the Task Force on Cannabis Legalization and Regulation
Foreword
When the Task Force first assembled in June 2016, we each brought a range of individual perspectives on cannabis. Over the months that followed, we came to appreciate the collective importance of our varied viewpoints and to recognize the potential impact of our work. This report is the result of a truly national collaboration, and we are proud to have been involved in it.
We have discovered that the regulation of cannabis will touch every aspect of our society. One of the predominant features of our deliberations has been the diversity of opinions, emotions and expertise expressed by those who came forward. People and organizations gave generously of their time and reflections. We explored the issue in remote corners of Canada as well as outside our borders. We heard from parents, patients, practitioners, politicians, police and the media. Our focus ranged from global treaty obligations to the homes and municipalities in which we live. We heard anxiety about such things as driving, youth access and “sending the wrong message,” but we also heard a desire to move away from a culture of fear around cannabis and to acknowledge the existence of more positive medical and social attributes. Meanwhile, as we went about our mandate, dispensaries continued to challenge communities and law enforcement, new research findings emerged, new regulations appeared, and the media shone their light on issues of quality and regulatory gaps.
Because of this complexity and diversity of input, and the challenges associated with designing a new regulatory framework, we recognize that there will be much discussion around the implications of our recommendations. However, like scraping ice from the car windows on a cold winter morning, we believe that we can now see enough to move forward.
The current paradigm of cannabis prohibition has been with us for almost 100 years. We cannot, and should not, expect to turn this around overnight. While moving away from cannabis prohibition is long overdue, we may not anticipate every nuance of future policy; after all, our society is still working out issues related to the regulation of alcohol and tobacco. We are aware of the shortcomings in our current knowledge base around cannabis and the effects of cannabis on human health and development. As a result, the recommendations laid out in this report include appeals for ongoing research and surveillance, and a flexibility to adapt to and respond to ongoing and emerging policy needs.
This report is a synthesis of Canadian values, situated in the times in which we live, combined with our shared experiences and concerns around a plant and its products that have touched many lives in many ways. For millennia, people have found ways to interact with cannabis for a range of medical, industrial, spiritual and social reasons, and modern science is only just beginning to unpack the intricacies of cannabinoid pharmacology. We are now shaping a new phase in this relationship and, as we do so, we recognize our stewardship not just of this unique plant but also of our fragile environment, our social and corporate responsibilities, and our health and humanity. This report is a beginning; we all have a role to play in the implementation of this new, transformative public policy.
In closing, we recognize and thank all those who contributed to our work, in particular our colleagues on the Task Force, the Secretariat and Eric Costen, who provided outstanding leadership. We formally acknowledge Prime Minister Justin Trudeau for his vision in initiating this process and for seeing it through. Finally, we thank the Ministers of Health, Justice and Public Safety for trusting us to prepare and deliver this report. On behalf of all Canadians, we now place our trust in our Government to enable and enact the processes required to make the legalization and regulation of cannabis a reality.
Anne McLellan
Chair
Mark A. Ware
Vice Chair
Ottawa, November 2016
Executive Summary
Introduction: Mandate, Context and Consultation Process
On June 30, 2016, the Minister of Justice and Attorney General of Canada, the Minister of Public Safety and Emergency Preparedness, and the Minister of Health announced the creation of a nine-member Task Force on Cannabis Legalization and Regulation (“the Task Force”). Our mandate was to consult and provide advice on the design of a new legislative and regulatory framework for legal access to cannabis, consistent with the Government’s commitment to “legalize, regulate, and restrict access.”
To fulfill our mandate, we engaged with provincial, territorial and municipal governments, experts, patients, advocates, Indigenous governments and representative organizations, employers and industry. We heard from many other Canadians as well, including many young people, who participated in an online public consultation that generated nearly 30,000 submissions from individuals and organizations. The Task Force looked internationally (e.g., Colorado, Washington State, Uruguay) to learn from jurisdictions that have legalized cannabis for non-medical purposes, and we drew lessons from the way governments in Canada have regulated tobacco and alcohol, and cannabis for medical purposes.
A Discussion Paper prepared by the Government, entitled “Toward the Legalization, Regulation and Restriction of Access to Marijuana,” informed the Task Force’s work and helped to focus the input of many of the people from whom we heard. The Discussion Paper identified nine public policy objectives. Chief among these are keeping cannabis out of the hands of children and youth and keeping profits out of the hands of organized crime. The Task Force set out guiding principles as the foundation of our advice to Ministers: protection of public health and safety, compassion, fairness, collaboration, a commitment to evidence-informed policy and flexibility.
In considering the experience of other jurisdictions and the views of experts, stakeholders and the public, we sought to strike a balance between implementing appropriate restrictions, in order to minimize the harms associated with cannabis use, and providing adult access to a regulated supply of cannabis while reducing the scope and scale of the illicit market and its social harms. Our recommendations reflect a public health approach to reduce harm and promote health. We also took a precautionary approach to minimize unintended consequences, given that the relevant evidence is often incomplete or inconclusive.
Minimizing Harms of Use
In taking a public health approach to the regulation of cannabis, the Task Force proposes measures that will maintain and improve the health of Canadians by minimizing the harms associated with cannabis use.
This approach considers the risks associated with cannabis use, including the risks of developmental harms to youth; the risks associated with patterns of consumption, including frequent use and co-use of cannabis with alcohol and tobacco; the risks to vulnerable populations; and the risks related to interactions with the illicit market. In addition to considering scientific evidence and input from stakeholders, the Task Force examined how other jurisdictions have attempted to minimize harms of use. We examined a range of protective measures, including a minimum age of use, promotion and advertising restrictions, and packaging and labelling requirements for cannabis products.
In order to minimize harms, the Task Force recommends that the federal government:
- Set a national minimum age of purchase of 18, acknowledging the right of provinces and territories to harmonize it with their minimum age of purchase of alcohol
- Apply comprehensive restrictions to the advertising and promotion of cannabis and related merchandise by any means, including sponsorship, endorsements and branding, similar to the restrictions on promotion of tobacco products
- Allow limited promotion in areas accessible by adults, similar to those restrictions under the Tobacco Act
- Require plain packaging for cannabis products that allows the following information on packages: company name, strain name, price, amounts of delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) and warnings and other labelling requirements
- Impose strict sanctions on false or misleading promotion as well as promotion that encourages excessive consumption, where promotion is allowed
- Require that any therapeutic claims made in advertising conform to applicable legislation
- Resource and enable the detection and enforcement of advertising and marketing violations, including via traditional and social media
- Prohibit any product deemed to be “appealing to children,” including products that resemble or mimic familiar food items, are packaged to look like candy, or packaged in bright colours or with cartoon characters or other pictures or images that would appeal to children
- Require opaque, re-sealable packaging that is childproof or child-resistant to limit children’s access to any cannabis product
- Additionally, for edibles:
- Implement packaging with standardized, single servings, with a universal THC symbol
- Set a maximum amount of THC per serving and per product
- Prohibit mixed products, for example cannabis-infused alcoholic beverages or cannabis products with tobacco, nicotine or caffeine
- Require appropriate labelling on cannabis products, including:
- Text warning labels (e.g., “KEEP OUT OF REACH OF CHILDREN”)
- Levels of THC and CBD
- For edibles, labelling requirements that apply to food and beverage products
- Create a flexible legislative framework that could adapt to new evidence on specific product types, on the use of additives or sweeteners, or on specifying limits of THC or other components
- Provide regulatory oversight for cannabis concentrates to minimize the risks associated with illicit production
- Develop strategies to encourage consumption of less potent cannabis, including a price and tax scheme based on potency to discourage purchase of high-potency products
- Require all cannabis products to include labels identifying levels of THC and CBD
- Enable a flexible legislative framework that could adapt to new evidence to set rules for limits on THC or other components
- Develop and implement factual public education strategies to inform Canadians as to risks of problematic use and lower-risk use guidance
- Conduct the necessary economic analysis to establish an approach to tax and price that balances health protection with the goal of reducing the illicit market
- Work with provincial and territorial governments to determine a tax regime that includes equitable distribution of revenues
- Create a flexible system that can adapt tax and price approaches to changes within the marketplace
- Commit to using revenue from cannabis as a source of funding for https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistration, education, research and enforcement
- Design a tax scheme based on THC potency to discourage purchase of high-potency products
- Implement as soon as possible an evidence-informed public education campaign, targeted at the general population but with an emphasis on youth, parents and vulnerable populations
- Co-ordinate messaging with provincial and territorial partners
- Adapt educational messages as evidence and understanding of health risks evolve, working with provincial and territorial partners
- Facilitate and monitor ongoing research on cannabis and impairment, considering implications for occupational health and safety policies
- Work with existing federal, provincial and territorial bodies to better understand potential occupational health and safety issues related to cannabis impairment
- Work with provinces, territories, employers and labour representatives to facilitate the development of workplace impairment policies
The Task Force further recommends that:
- In the period leading up to legalization, and thereafter on an ongoing basis, governments invest effort and resources in developing, implementing and evaluating broad, holistic prevention strategies to address the underlying risk factors and determinants of problematic cannabis use, such as mental illness and social marginalization
- Governments commit to using revenue from cannabis regulation as a source of funding for prevention, education and treatment
Establishing a Safe and Responsible Supply Chain
The cannabis supply chain includes production (including cultivation and manufacturing), distribution and retail. As part of our deliberations, we considered the most appropriate roles for the federal, provincial, territorial and local governments, given their areas of responsibility, capacity and experience. We were asked to give consideration to the participation of smaller producers, to the environmental impact of production, and to the regulation of industrial hemp under a new system. We heard about the pros and cons of different models for the retail market and about concerns regarding the sale of cannabis in the same location as alcohol or tobacco. We examined the question of personal cultivation in light of the experience of other jurisdictions, as well as the opinions of experts and the Canadian public.
To this end, the Task Force recommends that the federal government:
- Regulate the production of cannabis and its derivatives (e.g., edibles, concentrates) at the federal level, drawing on the good production practices of the current cannabis for medical purposes system
- Use licensing and production controls to encourage a diverse, competitive market that also includes small producers
- Implement a seed-to-sale tracking system to prevent diversion and enable product recalls
- Promote environmental stewardship by implementing measures such as permitting outdoor production, with appropriate security measures
- Implement a fee structure to recover https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative costs (e.g., licensing)
- Regulate CBD and other compounds derived from hemp or from other sources
The Task Force recommends that the wholesale distribution of cannabis be regulated by provinces and territories and that retail sales be regulated by the provinces and territories in close collaboration with municipalities. The Task Force further recommends that the retail environment include:
- No co-location of alcohol or tobacco and cannabis sales, wherever possible. When co-location cannot be avoided, appropriate safeguards must be put in place
- Limits on the density and location of storefronts, including appropriate distance from schools, community centres, public parks, etc.
- Dedicated storefronts with well-trained, knowledgeable staff
- Access via a direct-to-consumer mail-order system
The Task Force recommends allowing personal cultivation of cannabis for non-medical purposes with the following conditions:
- A limit of four plants per residence
- A maximum height limit of 100 cm on the plants
- A prohibition on dangerous manufacturing processes
- Reasonable security measures to prevent theft and youth access
- Oversight and approval by local authorities
Enforcing Public Safety and Protection
We believe that the new legal regime must be clear to the public and to law enforcement agencies, with enforceable rules and corresponding penalties that are proportional to the contravention.
In formulating our recommendations, we considered various ways of dealing with those who break the law and contravene rules, ranging from https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative to criminal sanctions. We were urged to avoid criminalizing youth. We looked at questions of personal possession limits and the public consumption of cannabis, and considered whether existing laws or a new law would provide the most appropriate legal framework for the new system.
We carefully considered the scientific and legal complexities surrounding cannabis-impaired driving, recognizing the concerns of Canadians about this issue. We learned of the various approaches used to address cannabis-impaired driving both in Canada and abroad, including the possibility of establishing a per se limit for THC – that is, a level deemed to be consistent with significant psychomotor impairment and increased risk of crash involvement. Our recommendations reflect the fact that the current scientific understanding of cannabis impairment has gaps and that more research and evidence, investments in law enforcement capacity, technology and tools, and comprehensive public education are needed urgently.
To this end, the Task Force recommends that the federal government:
- Implement a set of clear, proportional and enforceable penalties that seek to limit criminal prosecution for less serious offences. Criminal offences should be maintained for:
- Illicit production, trafficking, possession for the purposes of trafficking, possession for the purposes of export, and import/export
- Trafficking to youth
- Create exclusions for “social sharing”
- Implement https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative penalties (with flexibility to enforce more serious penalties) for contraventions of licensing rules on production, distribution, and sale
- Consider creating distinct legislation – a “Cannabis Control Act” – to house all the provisions, regulations, sanctions and offences relating to cannabis
- Implement a limit of 30 grams for the personal possession of non-medical dried cannabis in public with a corresponding sales limit for dried cannabis
- Develop equivalent possession and sales limits for non-dried forms of cannabis
The Task Force recommends that jurisdictions:
- Extend the current restrictions on public smoking of tobacco products to the smoking of cannabis products and to cannabis vaping products
- Be able to permit dedicated places to consume cannabis such as cannabis lounges and tasting rooms, if they wish to do so, with no federal prohibition. Safeguards to prevent the co-consumption with alcohol, prevent underage use, and protect health and safety should be implemented
With respect to impaired driving, the Task Force recommends that the federal government:
- Invest immediately and work with the provinces and territories to develop a national, comprehensive public education strategy to send a clear message to Canadians that cannabis causes impairment and that the best way to avoid driving impaired is to not consume. The strategy should also inform Canadians of:
- the dangers of cannabis-impaired driving, with special emphasis on youth; and
- the applicable laws and the ability of law enforcement to detect cannabis use
- Invest in research to better link THC levels with impairment and crash risk to support the development of a per se limit
- Determine whether to establish a per se limit as part of a comprehensive approach to cannabis-impaired driving, acting on findings of the Drugs and Driving Committee, a committee of the Canadian Society of Forensic Science, a professional organization of scientists in the various forensic disciplines
- Re-examine per se limits should a reliable correlation between THC levels and impairment be established
- Support the development of an appropriate roadside drug screening device for detecting THC levels, and invest in these tools
- Invest in law enforcement capacity, including Drug Recognition Experts and Standardized Field Sobriety Test training and staffing
- Invest in baseline data collection and ongoing surveillance and evaluation in collaboration with provinces and territories
The Task Force further recommends that all governments across Canada consider the use of graduated sanctions ranging from https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative sanctions to criminal prosecution depending on the severity of the infraction. While it may take time for the necessary research and technology to develop, the Task Force encourages all governments to implement elements of a comprehensive approach as soon as feasible, including the possible use of https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative sanctions or graduated licensing with zero tolerance for new and young drivers.
Medical Access
Canada’s medical cannabis regime was created and then shaped over time by the federal government’s response to successive court rulings regarding reasonable access. Today, medical cannabis falls within the purview of the Access to Cannabis for Medical Purposes Regulations (ACMPR).
In formulating our recommendations, we considered various aspects of access, including affordability, strains, potency, quality and adequacy of supply. We deliberated on the fundamental question of whether Canada should have a single system or two parallel systems, including separate access for medical cannabis. We also considered the strengths and weaknesses of the country’s current medical cannabis system and regulations.
We considered the views and experiences of patients and their advocacy organizations, the medical community, other jurisdictions and the public. While opinions of stakeholders may differ on some key questions, there is consensus on the need for more research aimed at understanding, validating and approving cannabis-based medicines.
In our view, the outcomes of such research will be necessary to determine the need for and features of a separate system for cannabis for medical purposes. However, as the new regulatory regime is established, it is important that the federal government continue to provide patients with reasonable access to cannabis for medical purposes, while contributing to the integrity of the overall cannabis regime and minimizing the potential for abuse and diversion.
To this end, the Task Force recommends that the federal government:
- Maintain a separate medical access framework to support patients
- Monitor and evaluate patients’ reasonable access to cannabis for medical purposes through the implementation of the new system, with action as required to ensure that the market provides reasonable affordability and availability and that regulations provide authority for measures that may be needed to address access issues
- Review the role of designated persons under the ACMPR with the objective of eliminating this category of producer
- Apply the same tax system for medical and non-medical cannabis products
- Promote and support pre-clinical and clinical research on the use of cannabis and cannabinoids for medical purposes, with the aim of facilitating submissions of cannabis-based products for market authorization as drugs
- Support the development and dissemination of information and tools for the medical community and patients on the appropriate use of cannabis for medical purposes
- Evaluate the medical access framework in five years
Implementation
The successful implementation of a regulatory framework for cannabis will take time and require that governments meet a number of challenges with respect to capacity and infrastructure, oversight, co-ordination and communications.
Capacity: Canada’s governments will need to move swiftly to increase or create capacity in many areas relating to the production and sale of cannabis. Success requires federal leadership, co-ordination and investment in research and surveillance, laboratory testing, licensing and regulatory inspection, training for law enforcement and others, and the development of tools to increase capacity ahead of regulation.
Oversight: To be satisfied that the system is minimizing harms as intended, it will need close monitoring and rapid reporting of results in a number of areas, including regulatory compliance and population health.
Co-ordination: The federal, provincial, territorial, municipal and Indigenous governments will need to work together on information and data sharing and co-ordination of efforts to set up and monitor all of the components of the new system. The Task Force believes that Canada should prioritize engagement of Indigenous governments and representative organizations, as we heard from Indigenous leaders about their interest in their communities’ participation in the cannabis market.
Communications: We heard from other jurisdictions about the importance of communicating early, consistently and often with the general public. Youth and parents will need the facts about cannabis and its effects. Actors in the new system – including employers, educators, law enforcement, industry, health-care practitioners and others – will require information tailored to their specific roles.
To this end, the Task Force recommends that the federal government:
- Take a leadership role to ensure that capacity is developed among all levels of government prior to the start of the regulatory regime
- Build capacity in key areas, including laboratory testing, licensing and inspection, and training
- Build upon existing and new organizations to develop and co-ordinate national research and surveillance activities
- Provide funding for research, surveillance and monitoring activities
- Establish a surveillance and monitoring system, including baseline data, for the new system
- Ensure timely evaluation and reporting of results
- Mandate a program evaluation every five years to determine whether the system is meeting its objectives
- Report on the progress of the system to Canadians
- Take a leadership role in the co-ordination of governments and other stakeholders to ensure the successful implementation of the new system
- Engage with Indigenous governments and representative organizations to explore opportunities for their participation in the cannabis market
- Provide Canadians with the information they need to understand the regulated system
- Provide Canadians with facts about cannabis and its effects
- Provide specific information and guidance to the different groups involved in the regulated cannabis market
- Engage with Indigenous communities and Elders to develop targeted and culturally appropriate communications
- Ensure that Canada shares its lessons and experience with the international community
These recommendations, taken together, present a new system of regulatory safeguards for legal access to cannabis that aim to better protect health and to enhance public safety. Their successful implementation requires the engagement and collaboration of a wide range of stakeholders. We believe that Canada is well-positioned to undertake the complex task of legalizing and regulating cannabis carefully and safely.
Chapter 1: Introduction
We begin our report by thanking those Canadians, experts, youth, Indigenous leaders, Elders, stakeholder organizations, government representatives, researchers, advocates, and patients, who took the time to participate in this consultation. Your views, advice and experiences have been insightful and invaluable.
We are thankful for the counsel provided by Mr. Bill Blair, the Parliamentary Secretary to the Minister of Justice, who served as Government liaison to the Task Force.
We are also grateful for the assistance and support provided by the federal Cannabis Legalization and Regulation Secretariat in helping us fulfill our mandate. Their continuous help with logistics, research, and communications gave us the freedom to focus on the content and meaning of the input received. We note our gratitude for the briefings provided by federal, provincial and territorial government officials to help guide our work. We would also like to note our appreciation for the support provided by the Canadian Consulates General in the states of Colorado and Washington during our study tours. Finally, we would like to thank Hill+Knowlton Strategies for their assistance in analyzing and synthesizing the nearly 30,000 submissions to the online questionnaire.
Our mandate
On June 30, 2016, the Minister of Justice and Attorney General of Canada, the Minister of Public Safety and Emergency Preparedness, and the Minister of Health announced the creation of a Task Force on Cannabis Legalization and Regulation (“the Task Force”). Comprised of nine Canadians of varied experience and backgrounds, the Task Force was given a mandate to consult and provide advice to the Government of Canada on the design of a new legislative and regulatory framework for legal access to cannabis, consistent with the Government’s commitment to “legalize, regulate, and restrict access” as set out in its December 2015 Speech from the Throne.
In carrying out this mandate, we were asked to engage with provincial, territorial and municipal governments, Indigenous governments and representative organizations, youth, patients and experts in relevant fields, including but not limited to: public health, substance use, criminal justice, law enforcement, economics and industry and those groups with expertise in production, distribution and sales of cannabis. The initial questions that formed the core of our consultations were elaborated for us in a Discussion Paper prepared by the Government, entitled “Toward the Legalization, Regulation and Restriction of Access to Marijuana” (Annex 4). This document proved to be a valuable resource in framing our early thinking, questions, and deliberations, as well as a stimulus for the thoughtful input we sought and received.
This report summarizes the views shared with the Task Force throughout our engagement activities and presents advice on a new system for regulated access to cannabis, responding to our mandate, the questions set out in the Discussion Paper and the issues that arose during our consultations.
The Canadian context
This Task Force report follows in the footsteps of earlier parliamentary exercises over the last 35 years that have considered questions regarding cannabis law reform in Canada: notably, in the early 1970s, the Commission of Inquiry into the Non-medical Use of Drugs (the Le Dain Commission); in 1996, the Standing Senate Committee on Legal and Constitutional Affairs; and, in 2002, the Senate Special Committee on Illegal Drugs. The reports published by these committees provided detailed analyses and recommendations that remain relevant today.
Canada has significant experience with cannabis use and cultivation. Despite the existence of serious criminal penalties for possessing, producing, and selling cannabis (cannabis possession offences account for half of all police-reported drug charges – 49,577 of 96,423 total in 2015), the Canadian Tobacco, Alcohol and Drugs Survey from 2015 found that 10% of adult Canadians (25 years and older) report having used cannabis at least once in the past year and over one-third reported using cannabis at least once in their lifetime. Additionally, Canadian youth are more likely to consume cannabis (in the past year, 21% of those aged 15-19, and 30% of those aged 20-24) than adult Canadians or their peers worldwide. In view of these statistics, it is unsurprising that cannabis is widely available throughout Canada and that a well-established cannabis market exists in Canada. Parallel to this illicit commercial market is a “cannabis culture,” which is a widespread and deep rooted network that emphasizes the social and cultural aspects of cannabis use and the sharing of information on its cultivation.
Canada’s experience with legal cannabis regulation can be attributed, at least in part, to successive court decisions over recent years which resulted in the evolution of a framework of legal access to cannabis for medical purposes. This model has evolved over the past two decades, from one that initially provided individual exemptions to enable medical patients to possess cannabis for their personal consumption, to a system of federal licensure that allows patients, with the support of their physicians, to obtain cannabis from a licensed producer, to cultivate their own cannabis, or to designate someone to cultivate it on their behalf. Taken together, our experiences with these approaches have enabled the establishment of a system of cannabis production and sale that informs our thinking around the regulation of cannabis for non-medical purposes.
A sophisticated commercial industry that cultivates and distributes cannabis by mail and courier to individuals who require it for medical purposes, and who are under the care of a physician or nurse practitioner, exists in Canada today, with 36 licensed producers in operation at the time of writing this report. This new industry operates under the authority of federal regulations (Access to Cannabis for Medical Purposes Regulations) which set out product quality control measures and strict security standards to protect public health and safety. Task Force members had the opportunity to visit some of these producers and were impressed by the sophistication and quality of their work.
Operating in parallel to this federally regulated system of commercial producers is a complex and varied illicit market.
There are those who operate complex organized criminal enterprises who engage in violence and pose a threat to the public safety and well-being of Canadians. Globally, organized criminal groups reap large profits from the proceeds of cannabis production and trafficking. Canada is an exporter of cannabis for global illicit markets.
There are also those who seek to exploit a period of transition wherein the Government has made clear its intent to change the laws but during which existing laws prohibiting illicit production and sale continue to apply. A lack of understanding among members of the public about what is and is not permitted during this period of transition has led to confusion that has contributed to the establishment and proliferation of illegal activities.
A network of cannabis growers, consumers and advocates who engage in an underground economy of cannabis cultivation and sale for compassionate reasons also exists. While these activities are in violation of the Controlled Drugs and Substances Act (CDSA) Footnote1, some cannabis stores (“dispensaries”) and wellness clinics (“compassion clubs”) have nevertheless been in operation for many years in parts of the country. The Task Force heard from several members of, and advocates for, this community who report developing and adhering to a strict internal code of standards, closely resembling self-regulation, and who wish to differentiate themselves from solely profit-driven, illicit enterprises.
A global perspective
Canada is one of more than 185 Parties to three United Nations drug control conventions: the 1961 Single Convention on Narcotic Drugs (as amended by the 1972 protocol), the 1971 Convention on Psychotropic Substances and the 1988 Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances.
Despite enforcement efforts under these treaties, cannabis remains the most widely used illicit drug in the world. Although the ultimate aim of the drug treaties is to ensure the “health and welfare of humankind,” there is growing recognition that cannabis prohibition has proven to be an ineffective strategy for reducing individual or social harms, including decreasing burdens on criminal justice systems, limiting negative social and public health impacts, and minimizing the entrenchment of illicit markets, which in some cases support organized crime and violence. Thus, a growing number of governments are interested in alternative approaches to cannabis control that promote and protect the health, safety and human rights of their populations. Several European and Latin American countries have decriminalized the personal possession of cannabis.
This global shift in approaches to controlling and minimizing the harms associated with cannabis use has, for some, gone further. In 2013, Uruguay became the first country to enact legislation to legalize and regulate cannabis for non-medical purposes. At the sub-national level, following the United States [U.S.] federal election on November 8, 2016, a total of eight U.S. states – Alaska, California, Colorado, Maine, Massachusetts, Nevada, Oregon and Washington – and the District of Columbia – have now voted to legalize and regulate cannabis for non-medical purposes. These states represent more than 20% of the total U.S. population (approximately 75 million people).
While it is not part of the Task Force’s mandate to make recommendations to the Government on how to address its international commitments, it is our view that Canada’s proposal to legalize cannabis shares the objectives agreed to by member states in multilateral declarations, namely: to protect vulnerable citizens, particularly youth; to implement evidence-based policy; and to put public health, safety and welfare at the heart of a balanced approach to treaty implementation.
Important lessons will undoubtedly arise from Canada’s experience in the coming years, ones that will be valuable for advancing the global dialogue on innovative strategies for drug control. We believe that Canada will remain a committed international partner by monitoring and evaluating our evolving cannabis policy and sharing these important lessons with national and international stakeholders.
Setting the frame
The mandate entrusted to us was to design a framework with new rules that would define and set the parameters for how Canadians access cannabis in the future.
Defining the terms
Legalization and regulation must be distinguished from “decriminalization,” as the terms are easily confused. Generally, decriminalization is referred to as removing criminal sanctions for some offences, usually simple possession, and replacing them with https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative sanctions, such as fines. This maintains the illegality of cannabis but prevents individuals from acquiring a criminal record for simple possession. With decriminalization the production Footnote2, distribution and sale of cannabis remain criminal activities. Thus, individuals remain subject to the potential dangers of untested cannabis. Criminal organizations continue to play the role of producer, distributor and seller, thereby increasing risk, particularly to vulnerable populations.
Cannabis versus marijuana
The word “marijuana” is a common term used most often in reference to the dried flowers and leaves of the cannabis plant. It is a slang term that is not scientifically precise. We believe it is more appropriate to use the term cannabis when engaging in a serious discussion of the goals and features of a new regulatory system for legal access.
Indeed, Cannabis sativa is the botanical name for this ubiquitous herbaceous plant, which includes the drug type (“marijuana”) as well as industrial hemp.
Public policy objectives
The Honourable Jane Philpott, Minister of Health, during her plenary statement for the Special Session of the United Nations General Assembly on the World Drug Problem, outlined that “our approach to drugs must be comprehensive, collaborative and compassionate. It must respect human rights while promoting shared responsibility.” Footnote3
In moving ahead with its commitment to legalize, regulate and restrict access to cannabis, the Government set out its principal objectives in its Discussion Paper. These objectives were established to:
- Protect young Canadians by keeping cannabis out of the hands of children and youth;
- Keep profits out of the hands of criminals, particularly organized crime;
- Reduce the burdens on police and the justice system associated with simple possession of cannabis offences;
- Prevent Canadians from entering the criminal justice system and receiving criminal records for simple cannabis possession offences;
- Protect public health and safety by strengthening, where appropriate, laws and enforcement measures that deter and punish more serious cannabis offences, particularly selling and distributing to children and youth, selling outside of the regulatory framework, and operating a motor vehicle while under the influence of cannabis;
- Ensure Canadians are well-informed through sustained and appropriate public health campaigns and, for youth in particular, ensure that risks are understood;
- Establish and enforce a strict system of production, distribution and sales, taking a public health approach, with regulation of quality and safety (e.g., child-proof packaging, warning labels), restriction of access, and application of taxes, with programmatic support for addiction treatment, mental health support and education programs;
- Provide access to quality-controlled cannabis for medical purposes consistent with federal policy and court decisions;
- Enable ongoing data collection, including gathering baseline data, to monitor the impact of the new framework.
Paramount among these objectives are those intended to keep cannabis out of the hands of children and youth and to keep profits out of the hands of organized crime. Many have remarked that there is an inherent tension between these objectives. On the one hand, establishing a system with adequate protections that would seek to curb access to cannabis by youth suggests adopting a more restrictive model with numerous controls and safeguards, such as establishing higher age limits, adapting pricing strategies to discourage consumption, and imposing limitations to minimize promotion and commercialization. On the other hand, seeking to displace the illicit cannabis market requires the establishment of a legal market that is competitive with the existing illicit market, including safe and reasonable access, price, variety of product choice and adequate consumer education. Therefore, excessive restrictions could lead to the re-entrenchment of the illicit market. Conversely, inadequate restrictions could lead to an unfettered and potentially harmful legal market. Both extremes jeopardize the viability of the new system for cannabis.
The different approaches to regulating popular, yet potentially harmful and addictive, substances are well illustrated by how Canadian society has, over several decades, approached tobacco and alcohol. In this time, tobacco has moved from being heavily marketed to being highly restricted, whereas alcohol has moved from being strictly controlled to being widely available and promoted.
We were told on many occasions that we need to find a balance for cannabis. The diagram in Figure 1 below helps to illustrate the spectrum of options shown against a curve of potential harms, where at one end prohibition leads to thriving criminal markets and at the other unregulated, legal free markets lead to unrestrained commercialization. At both extremes, there exist social and health harms that most Canadians would find unacceptable.
At the bottom of the curve lies the balance we are seeking with regard to cannabis: the point on the continuum where the public policy goals set out by the Government are most likely to be achieved.
Figure 1 Footnote4 A spectrum of options

Figure 1 description
In seeking this balance, we believe that it is necessary to adopt a public health approach. As such, our recommendations are shaped by our view that the decisions taken in determining the precise features of this new regulatory system should uphold and promote the health of Canadians while reducing harms. In our discussions with experts, governments and others, strong support emerged for this public health approach, which includes:
- A focus on reducing harm and promoting health at the population level;
- Targeted interventions for high-risk individuals and practices;
- A concern with fairness;
- An evidence-based approach.
While it is well within the authority of governments to choose to apply taxes, to collect appropriate licensing fees and to establish cost-recovery systems, it is also our view that revenue generation should be a secondary consideration for all governments, with the protection and promotion of public health and safety as the primary goals.
Our advice is informed by the available evidence
Ideally, all of our recommendations would be based on clear, well-documented evidence. However, we recognize that cannabis policy, in its many dimensions, lacks comprehensive, high-quality research in many areas. On many issues throughout our discussions and deliberations, we have found that evidence is often non-existent, incomplete or inconclusive.
Being mindful of these limitations is imperative. It is more appropriate to refer to our recommendations as “evidence-informed” rather than “evidence-based”, given that the relationship between evidence and policy is complex and that our recommendations were influenced by the concerns, priorities and values expressed by stakeholders and members of the public, as well as by the available scientific evidence.
Moreover, a clear reality underpins our discussions and deliberations: encouraging and enabling more research and ensuring systematic monitoring, evaluation and reporting on our experiences is essential to good public policy in this area.
Some of these concepts are explored in greater detail in the section below, which describes the guiding principles behind our advice.
Engagement process
Fulfilling our mandate required that we seek as many views as possible from a diverse and informed community of experts, professionals, advocates, front-line workers, policy makers, government officials, patients, citizens and employers in the time provided to us. With this in mind, early in our work we identified a strategy for engagement that would rely upon various methods and means to reach out to Canadians and hear their views:
- Canadians: An online portal was open to the public for 60 days throughout July and August of 2016 and received nearly 30,000 submissions to the questions posed. Demographic information on the respondents is set out in Annex 5. The number of responses we received is clear evidence that many Canadians hold strong views on this subject, and we benefitted greatly from their collective views and advice. Hill+Knowlton Strategies assisted the Task Force in its analysis and synthesis of the responses. A summary of its report is included in Annex 5.Moreover, nearly 300 written submissions were submitted to the Task Force from various organizations. These submissions were often comprehensive presentations of the main issues of concern. A complete list of all the organizations and individuals who provided submissions is included in Annex 3.
- Governments: A key requirement in our mandate was to engage with provincial and territorial governments. We travelled to most provincial capital cities and to the North where we met with government officials representing multiple sectors and ministries. We participated in candid discussions and gained a clearer understanding of the diverse regional realities that will influence public policy in this area.
- Experts: We hosted a series of roundtable discussions in cities across the country, in order to engage with experts from a wide spectrum of disciplines, researchers and academics, patients and their advocates, cannabis consumers, chiefs of police and fire departments, and other municipal and local government officials, as well as numerous industry, professional, health and other associations.
- Indigenous peoples: Indigenous experts, representative organizations, governments and Elders were invited to participate in a variety of Task Force engagement activities, including in the expert roundtables, bilateral meetings and an Indigenous peoples roundtable. These opportunities provided the Task Force with valuable perspectives and a better understanding of the interests and concerns of First Nations, Inuit and Métis communities.
- Youth: Youth are at the centre of the Government’s objectives in pursuing a new system of regulated legal access to cannabis. Their voices were therefore essential. The Task Force sought to engage youth by including them and youth-serving organizations in expert roundtables and by hosting a youth-focused roundtable. The Task Force would also like to acknowledge Canadian Students for Sensible Drug Policy for their work in convening a youth roundtable event as a direct contribution to the Task Force’s youth engagement activities.
- Patients: Access to cannabis for medical purposes is a major preoccupation for many Canadian patients, their families, caregivers and health-care providers. The emergence of a regulatory framework for non-medical cannabis access was seen by many to be a challenge to medical cannabis access, products and research. We are grateful to Canadians for Fair Access to Medical Marijuana, the Arthritis Society, the Canadian AIDS Society, and the British Columbia Compassion Club Society for helping to facilitate a roundtable for patients.
- Study tours: In order to learn first-hand from those who have legalized cannabis, the Task Force conducted site visits to Colorado and Washington states. We were hosted by state officials and we participated in a range of briefings, meetings and site visits. Similarly, senior officials from the Government of Uruguay provided a detailed briefing to the Task Force regarding Uruguay’s unique experience as the only country to date to have enacted a regulatory system for legal access to cannabis.
The Task Force visited some of Canada’s licensed producers of cannabis, in order to understand the realities of regulated cannabis production in Canada. We also visited the B. C. Compassion Club Society, in order to learn from its experience of providing cannabis in a holistic, wellness-centered environment to patients in Vancouver for the last two decades.
The Task Force acknowledges that we were not able to hear from everyone who wished to offer their views. However, we are confident that we heard a diversity of views on the central issues in question. Our advice in this report is informed, and shaped, by the perspectives, knowledge and experiences shared with us by so many. A list of persons and organizations consulted can be found in Annex 3.
Guiding principles
Given the complexity of the issues, the Task Force set out a series of guiding principles and values that we see as important building blocks for our recommendations. The following principles and values have been validated throughout our consultations:
- Protection of public health and safety as the primary goal of the new regulatory framework, which includes minimizing harms and maximizing benefits;
- Compassion for vulnerable members of society and patients who rely on access to cannabis for medical purposes;
- Fairness in avoiding disproportionate or unjustified burdens to particular groups or members of society and in avoiding barriers to participation in the new framework;
- Collaboration in the design, implementation, and evaluation of the new framework, including communication and collaboration among all levels of government and with members of the international community;
- Commitment to evidence-informed policy and to research, innovation, and knowledge exchange;
- Flexibility in implementing the new framework, acknowledging that there is much we do not know and much that we will learn over time.
Chapter 2: Minimizing Harms of Use
Introduction: a public health approach
In taking a public health approach to the regulation of cannabis, the Task Force proposes measures that will maintain and improve the health of Canadians by minimizing the harms associated with cannabis use.
Most of the measures we propose seek to minimize harms in the population as a whole. We also consider more targeted means to minimize the harm to individuals, particularly children, youth and other vulnerable populations. A discussion of the harms associated with cannabis-impaired driving can be found in Chapter 4, Enforcing Public Safety and Protection.
Based on evidence that the risks of cannabis are higher with early age of initiation and/or high frequency of use, the Task Force proposes a public health approach that aims to:
- Delay the age of the initiation of cannabis use;
- Reduce the frequency of use;
- Reduce higher-risk use;
- Reduce problematic use and dependence;
- Expand access to treatment and prevention programs; and,
- Ensure early and sustained public education and awareness.
Cannabis: the essentials
Cannabis sativa is a plant that is used for its psychoactive and therapeutic effects and, like all psychoactive and therapeutic substances, carries certain risks to human health. Cannabis contains hundreds of chemical substances and more than 100 cannabinoids, which are compounds traditionally associated with the cannabis plant. Among these, two cannabinoids have received the most scientific interest: delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD). THC has therapeutic effects and is the compound chiefly responsible for the psychoactive effects of cannabis, while CBD has potential therapeutic but no obvious psychoactive effects. The effects of cannabis are due to the actions of its cannabinoids on biological “targets,” a system of specific receptors and molecules found throughout the human body, together called the endocannabinoid system. The current science also suggests that other compounds in cannabis, such as aromatic terpenes and flavonoids, may also have pharmacological properties alone or in combination with the cannabinoids.
Assessing the risks
Risk is inherent in all discussions on the health effects of cannabis, yet our understanding of risk is constrained by more than 90 years of prohibition, which has limited our ability to fully study cannabis.
We know more about the short-term effects of cannabis use (e.g., psychoactive effects and effects on memory, attention and psychomotor function). We are less certain about some of the longer-term effects (e.g., risks of permanent harms to mental functioning and risks of depression and anxiety disorders) but more certain about others (e.g., dependence). The following is a snapshot of the risks of harms associated with cannabis use:
- Risks to children and youth: Generally speaking, studies have consistently found that the earlier cannabis use begins and the more frequently and longer it is used, the greater the risk of potential developmental harms, some of which may be long-lasting or permanent.
- Risks associated with consumption: Certain factors are associated with an increased risk of harms, including frequent use and use of higher potency products. Driving while impaired by cannabis is associated with an increased risk of accidents and fatalities. Co-use with alcohol may pose an incremental risk for impaired driving and co-use with tobacco may increase smoking-related lung disease.
- Risks to vulnerable populations: Studies have found associations between frequent cannabis use and certain mental illnesses (e.g., schizophrenia and psychosis) and between frequent cannabis use during pregnancy and certain adverse cognitive and behavioural outcomes in children.
- Risks related to interactions with the illicit market: These include violence and the risks associated with unsafe products, illicit production and exposure to other, more harmful illicit substances.
As noted in Chapter 1, in addressing these risks we are sometimes faced with trade-offs when choosing among different regulatory approaches, since reducing some risks could result in increasing others. We often turned to our guiding principles to help us make difficult choices.
In our roundtable discussions and throughout the submissions we received, stakeholders often noted that, alongside the risks of use, there are also benefits, including for relaxation purposes, as a sleep aid or for pleasure. Notably, there is emerging evidence with regard to the use of cannabis as an alternative to more harmful substances, suggesting a potential for harm reduction (see also Chapter 5, Medical Access). The Task Force agrees that further research should be a priority.
Learning from the regulation of tobacco and alcohol
In assessing the measures presented in this chapter, at times comparisons are made with the ways alcohol and tobacco are regulated. In some ways the substances are comparable, being associated with factors such as impairment, dependence, health harms and widespread use. However, there are important differences in risks, social and health impact, and prevalence of use.
The 2009 World Health Organization (WHO) ranking of leading global risk factors for disease includes alcohol (ranked 3rd) and tobacco (6th). Notably, it does not include cannabis. In comparing levels of risk, it is important to consider patterns of use and the high global prevalence of alcohol and tobacco use. As well, years of research data collection and evaluation have provided information on the individual and societal impacts of alcohol and tobacco use that is not yet available for cannabis. Nevertheless, the Task Force acknowledges that, based on current levels of use and available information on mortality and morbidity, the harms associated with the use of tobacco or alcohol are greater than those associated with the use of cannabis.
In this report we recommend a series of measures that are, in some cases, stricter than those that exist for tobacco or alcohol in Canada. Given the relative harms, we acknowledge this contradiction but believe that the regulation of these substances has been inconsistent with WHO disease risk ranking and remains inconsistent with known potential for harm. In designing a regulatory system for cannabis, we have an opportunity to avoid similar pitfalls.
The Task Force recognizes that the regulatory regimes for alcohol and tobacco continue to evolve. It is our hope that our experience with cannabis regulation will be used to inform the further evolution of alcohol and tobacco regulations.
Minimum age
Setting a minimum age for the purchase of cannabis is an important requirement for the new system. The age at which to set the limit was the subject of much discussion and analysis throughout our deliberations.
As with many of the other measures discussed in this chapter, a minimum age is intended to support the Government’s objective to protect children and youth from the potential adverse health effects of cannabis by putting in place safeguards that better control access. In Canada, minimum ages for alcohol and tobacco sales have been set by the federal government (for tobacco) and by the provinces and territories (for both substances). Some have set the legal age for purchase at 18, others at 19. However, we know that age restrictions on their own will not dissuade youth use; other complementary actions – including prevention, education, and treatment – are required to achieve this objective.
What we heard
The Task Force heard broad support for establishing a minimum age for the sale of cannabis. However, the youth with whom we spoke did not believe that setting a minimum age alone would prevent their peers from using cannabis.
Some health experts argued that there was no clear scientific evidence to identify a “safe” age of consumption, but agreed that having a minimum age would reduce harm. There was a general recognition that a minimum age for cannabis use would have value as a “societal marker,” establishing cannabis use as an activity for adults only, at an age at which responsible and individual decision-making is expected and respected.
We heard from many participants that setting the minimum age too high risked preserving the illicit market, particularly since the highest rates of use are in the 18 to 24 age range. A minimum age that was too high also raised concerns of further criminalization of youth, depending on the approach to enforcement.
Ages 18, 19 and 21 were most often suggested as potential minimum ages. Health-care professionals and public health experts tend to favour a minimum age of 21. A minimum age of 25, often cited as the age at which brain development has stabilized, was generally viewed as unrealistic because it would leave much of the illicit market intact. In U.S. states where cannabis is legal, governments have aligned the minimum age at 21 for alcohol and cannabis consumption.
There was considerable discussion regarding the importance of national consistency. Having the same minimum age for purchase in all provinces and territories was thought to mitigate problems associated with “border shopping” by youth seeking to purchase cannabis in a neighbouring province or territory where the age is lower. In this regard, we heard suggestions that governments could learn from the challenges associated with alcohol age limits, which are inconsistent across the country. A range of public health and other experts recommended that the federal government set the minimum age, and that the provinces and territories be able to raise the age but not lower it.
Others argued that, for the sake of clarity and symmetry, the minimum age for purchasing cannabis should be aligned with the current provincial and territorial ages for sales of alcohol and tobacco. Many suggested that 18 was a well-established milestone in Canadian society marking adulthood.
Considerations
Research suggests that cannabis use during adolescence may be associated with effects on the development of the brain. Use before a certain age comes with increased risk. Yet current science is not definitive on a safe age for cannabis use, so science alone cannot be relied upon to determine the age of lawful purchase.
Recognizing that persons under the age of 25 represent the segment of the population most likely to consume cannabis and to be charged with a cannabis possession offence, and in view of the Government’s intention to move away from a system that criminalizes the use of cannabis, it is important in setting a minimum age that we do not disadvantage this population.
There was broad agreement among participants and the Task Force that setting the bar for legal access too high could result in a range of unintended consequences, such as leading those consumers to continue to purchase cannabis on the illicit market.
For these reasons, the Task Force is of the view that the federal government should set a minimum age of 18 for the legal sale of cannabis, leaving it to provinces and territories to set a higher minimum age should they wish to do so.
To mitigate harms between the ages of 18 and 25, a period of continued brain development, governments should do all that they can to discourage and delay cannabis use. Robust preventive measures, including advertising restrictions and public education, all of which are addressed later in this chapter, are seen as key to discouraging use by this age group.
For many in the legal and law enforcement fields, the key issue is not the minimum age itself but the implications for those who ignore it, including those who sell to children and youth, and those under the minimum age who possess and use cannabis. These are addressed in Chapter 4, Enforcing Public Safety and Protection.
Advice to Ministers
The Task Force recommends that the federal government set a national minimum age of purchase of 18, acknowledging the right of provinces and territories to harmonize it with their minimum age of purchase of alcohol.
Promotion, advertising and marketing restrictions
In designing a system for the regulation of cannabis, we are creating a new industry. As with other industries, this new cannabis industry will seek to increase its profits and expand its market, including through the use of advertising and promotion. Because of the risks discussed earlier in this chapter, regulation aims to discourage use among youth and ensure that only evidence-informed information is provided to adults. Restrictions on advertising, promotion and related activities are therefore necessary.
Our society’s experience with the promotion of tobacco and alcohol is instructive, since the promotion of these products is recognized as an important driver of consumption and of the associated harms. In response, many governments have restricted how tobacco and alcohol may be promoted. In Canada, there are different approaches to each.
The federal Tobacco Act restricts the promotion of tobacco products, except in limited circumstances. It also specifically prohibits promotion by means of a testimonial or endorsement, false or misleading advertising, sponsorship promotion, lifestyle advertising (which evokes images of glamour, excitement, and risk) and advertising appealing to young people.
Advertising that promotes a tobacco product by describing brand characteristics or providing information (factual information about a product and its characteristics, availability or price) are permitted in limited circumstances, such as in publications and in locations not accessible to young people. Provincial and territorial laws also set stringent limits on promotion of tobacco products.
The Canadian Radio-television and Telecommunications Commission’s Code for Broadcast Advertising of Alcoholic Beverages includes federal restrictions on the promotion of alcohol in radio and television broadcasting. It includes prohibitions on advertisements that appeal to minors, that encourage the general consumption of alcohol and that associate alcohol with social or personal achievement. Each province and territory also has its own rules restricting the promotion of alcohol. Despite regulations such as the advertising code, alcohol is heavily marketed and promoted to adults in Canada.
What we heard
In the Task Force’s consultations, the majority of health-care professionals, as well as public health, municipal, law enforcement and youth experts, believed there should be strict controls on advertising and marketing of cannabis. We heard that such restrictions would be necessary to counter the efforts by industry to promote consumption, particularly among youth. There were also concerns expressed that companies would market products to heavy users or encourage heavy use, and exploit any exceptions that are left open.
We heard strong support from, among others, educators, parents, youth and the public health community for comprehensive marketing restrictions for cannabis similar to those for tobacco. Such restrictions were considered to be necessary because the evidence from our experience with tobacco and alcohol suggests that partial restrictions send mixed messages about use.
Several public health stakeholders also recommended plain packaging for cannabis products, similar to the approach taken by Australia for tobacco products and which are soon to be applied to tobacco products in Canada. Plain packaging refers to packages without any distinctive or attractive features and with limits on how brand names are displayed (e.g., font type, colour and size).
The industry representatives from whom we heard, while generally supportive of some promotion restrictions – particularly marketing to children and youth, and restrictions on false or misleading advertising – made the case for allowing branding of products. It was suggested that brand differentiation would help consumers distinguish between licit and illicit sources of cannabis, helping to drive them to the legal market. As well, to achieve “brand loyalty,” companies would have the impetus to produce high-quality products and would be more accountable to their customers.
In our online consultation, some were opposed to tobacco-style advertising restrictions for cannabis because, in their opinion, cannabis is less harmful than either tobacco or alcohol.
For some online respondents, allowing in-store advertising for cannabis brands offered a potential compromise: youth would be protected from exposure to mass marketing and advertising, while producers and retailers could still engage and communicate with consumers of cannabis of legal age and in regulated environments.
Considerations
The Task Force agrees with the public health perspective that, in order to reduce youth access to cannabis, strict limits should be placed on its promotion. In our view, comprehensive restrictions similar to those created by tobacco regulation offer the best approach. There is also a concern that the presence of any cannabis promotion could work against youth education efforts.
The challenges with creating partial restrictions (i.e., only prohibiting advertising targeting youth) are well documented. In practice, it is difficult to separate marketing that is particularly appealing to youth from any other marketing. The Colorado officials with whom we met echoed this concern, noting that their partial restrictions for cannabis advertising made it challenging to avoid advertising that reaches, or is appealing to, youth.
A partial restriction focusing on marketing to youth becomes even more problematic if one considers the 19-to-25 age group; it will be legal for those in this age group to purchase, but the evidence of potential harm suggests that use within this group should be discouraged as a matter of health. Trying to prohibit marketing that is appealing to this age group compared to people in their late 20s or 30s would be impossible. The Task Force believes that, while there should be a federal minimum age of 18 for the reasons explained above, other policies, such as comprehensive marketing restrictions, will be needed to minimize harms to the 18-to-25 age group.
Comprehensive advertising restrictions should cover any medium, including print, broadcast, social media, branded merchandise, etc., and should apply to all cannabis products, including related accessories. Such restrictions could still leave room for promotion at the point of sale, which would answer industry concerns about allowing information to be provided to consumers and some branding to differentiate their products from the illicit market and other producers. This assumes that the point of sale is a retail outlet not accessible to minors (see Chapter 3, Establishing a Safe and Responsible Supply Chain); the Tobacco Act allows information and brand preference advertising in places where young persons are not permitted, and those provisions could be used as a model.
If branding were permitted, along with limited point-of-sale marketing and product information, we are concerned that this information would still make its way to environments where minors would be exposed and influenced, much as they are today by alcohol and tobacco brands. The Task Force feels there is sufficient justification at this time for plain packaging on cannabis products. Such packaging would include the company name, as well as important information for the consumer, including price and strain name, as well as any applicable labelling requirements (see the “Cannabis-based edibles and other products” and “THC potency” sections in this chapter).
Any promotion, marketing or branding that is allowed should still be subject to restrictions, such as lifestyle advertising (similar to the Tobacco Act restrictions), false or misleading promotion (as for food, drugs and any other consumer product), the encouragement of excessive consumption (similar to standards for alcohol) and therapeutic claims (similar to restrictions for drugs or natural health products in the Food and Drugs Act).
In setting restrictions, the federal government should consider options for oversight and enforcement. This should include effective oversight by government, possibly supplemented by industry self-regulation (as is the case with pharmaceuticals). Advice on the appropriate penalties for those companies that violate these requirements is outlined in Chapter 4.
Advice to Ministers
The Task Force recommends that the federal government:
- Apply comprehensive restrictions to the advertising and promotion of cannabis and related merchandise by any means, including sponsorship, endorsements and branding, similar to the restrictions on promotion of tobacco products
- Allow limited promotion in areas accessible by adults, similar to those restrictions under the Tobacco Act
- Require plain packaging for cannabis products that allows the following information on packages: company name, strain name, price, amounts of THC and CBD and warnings and other labelling requirements
- Impose strict sanctions on false or misleading promotion as well as promotion that encourages excessive consumption, where it is allowed
- Require that any therapeutic claims made in advertising conform to applicable legislation
- Resource and enable the detection and enforcement of advertising and marketing violations, including via traditional and social media
Cannabis-based edibles and other products
In observing the manner in which illicit and legal markets for cannabis have emerged and continue to evolve, it is clear that cannabis is a versatile raw material that can be used to make a wide variety of consumer, medicinal and industrial products. Extending far beyond the dried cannabis popularized in the 1960s and 1970s, today’s cannabis is available in a wide range of cannabis-infused foods, cooking oils and drinks (typically referred to as “edibles”), oils, ointments, tinctures, creams and concentrates (e.g., butane hash oil, resins, waxes, and “shatter”). These products can be made with different types of cannabis, with varying levels of THC and CBD, resulting in different intensities and effects. The net result is that any discussion about regulating a new cannabis industry quickly leads to an understanding of the complexity of regulating not one but potentially thousands of new cannabis-based products.
Under Canada’s current cannabis for medical purposes system, the Government permits only dried and fresh cannabis and cannabis oils. Although other cannabis products may not be sold, the regulations allow individuals to make edible products, such as baked goods, for their own consumption. Nevertheless, access to a broad range of cannabis products is possible via the illicit market, including through dispensaries and online retailers. Determining the extent to which the new regulatory system should enable or restrict the range of legally accessible cannabis products, both initially as well as over the longer term, and whether and how to limit the availability of cannabis and cannabis products with high levels of THC (see “THC potency,” later in this chapter) are critical issues.
Edible products have emerged as a focal point in our discussions, given their variety and increasing popularity, as well as their particular risks.
What we heard: Cannabis-based edibles
Since legalizing cannabis, the states of Colorado and Washington have seen sustained growth in their cannabis edibles markets. In Colorado, sales of cannabis-infused edibles in the first quarter of 2015 were up 134% from the same period in the previous year.
Colorado officials acknowledge that a lack of regulation around edibles in the early days of legalization led to some unintended public health consequences. Their experience provides the Task Force with a number of specific “lessons learned”:
- Expect edibles to have a broad appeal. Cannabis products such as brownies, cookies and high-end chocolates are attractive to novice users and those who do not want to smoke or inhale. Colorado’s prohibition on public smoking also gave a boost to the edibles market.
- Control for level of THC and/or portion size. In some respects, it is easier to control the amount of THC ingested when smoked or vaporized compared to when it is eaten. This is because, unlike the more immediate euphoric and other psychoactive effects produced by smoking or vaporizing cannabis, it can take several hours for THC given orally to take full effect. In Colorado, this has sometimes resulted in accidental overconsumption and overdoses. (A cannabis overdose is not known to be fatal, but can be unpleasant and potentially dangerous – including severe anxiety, nausea, vomiting, a psychotic episode, or hypotension and loss of consciousness.) Controlling the amount of THC (or other cannabinoids) in a product, as well as establishing a standardized serving size, is important to avoid or limit such incidents.
- Ensure that cannabis edibles can be clearly distinguished. It can be a challenge to differentiate between cannabis edibles and cannabis-free products, leading to a risk that individuals, including children, inadvertently consume them. Since legalization of cannabis, Colorado and Washington have seen an increase in calls to poison control lines and in emergency room visits.
On the basis of the risk of exposure to children, and also the potential of edibles to broaden the appeal of cannabis products, public health stakeholders have advocated to the Task Force that edibles not be allowed under a regulated system. For example, we were informed that of the 1,969 cases of cannabis exposures in children under the age of six reported in the National Poison Data System in the United States between 2000 and 2013, 75% were exposed through ingestion.
However, there are a number of points to consider in this regard. The period in question largely pre-dates the wider regulation of cannabis in Colorado in 2012 and regulatory changes in 2014 (see below). And, despite the rise in rates, the absolute number of reported poisonings remains a small proportion of all reports: calls to Washington’s poison control line related to cannabis exposure (mostly in teens) in 2015 were 0.4% of all calls to the line.
Many submissions to the Task Force suggested that Canada could learn from the way U.S. states have responded to ingestion incidents. In 2014, Colorado set out new requirements for the sale of all edible cannabis products, including:
- A standard serving size (10 mg of THC or less) clearly demarked on every product;
- A maximum amount of THC per unit of product;
- Clear labelling of amount of THC on packages; and,
- Child-resistant, opaque and re-sealable packaging.
Such requirements have become the best practice for other U.S. states that have legalized, although the serving size can vary (and is typically higher for medical products). In October 2016, Colorado took further steps to improve the safety of packaging of edibles by requiring that all standardized servings be imprinted with a symbol containing the letters THC and prohibiting packaging that appeals to children.
Among stakeholders, the Task Force heard several arguments in favour of allowing and regulating edibles, including:
- Providing a potentially safer alternative to smoking cannabis;
- Making THC oil (the active ingredient in edibles) can be a dangerous process and should only be done in controlled facilities and not in residential areas;
- Having users create their own edibles with cannabis oil could lead to uneven distribution of THC in the product, resulting in a potential for overdose; and
- Regulation would allow for quality control over products, and for appropriate education and in-store information.
Considerations
In the illicit cannabis market, governments face an entrenched, sophisticated market that offers a wide range of cannabis products with no oversight and in which consumers are vulnerable to all the risks associated with unregulated products.
In weighing the arguments for and against limitations on edibles, the majority of the Task Force concluded that allowing these products offers an opportunity to better address other health risks. Edible cannabis products offer the possibility of shifting consumers away from smoked cannabis and any associated lung-related harms. This is of benefit not just to the user but also to those around them who would otherwise be subject to second-hand smoke.
This position comes with caveats. To protect the most vulnerable, any products that are “appealing to children,” such as candies and other sweets, should be prohibited. We acknowledge that there is considerable discretion in what constitutes “appealing to children.” The Government may want to consider the approach taken by the Alaskan government, which prohibits the manufacture and sale of any cannabis product that “closely resembles a familiar food or drink item including candy,” or is “adulterated” with additives or sweeteners. We are confident that with clear guidance to industry by the regulator and vigilant and predictable enforcement this is not an insurmountable barrier.
The Task Force is concerned by the reports of an increase of accidental ingestion by children in states where cannabis is legal. We acknowledge that a lack of regulation contributed to this risk. Should edibles be allowed for legal sale in Canada, they should, at a minimum, conform to the strictest packaging and labelling requirements for edibles currently in force in U.S. states. Since these measures are fairly recent, the markets (Canadian and U.S.) should be closely monitored to determine the effectiveness of these measures.
In the event that future research and monitoring identifies new risks with existing or new cannabis products, including increases in use, the Government should be ready to react. The system must be flexible enough to adapt in a timely way to new information and to provide appropriate safeguards as evidence indicates.
What we heard: Other products
Participants raised concerns about the development of products that combine cannabis with other harmful substances, especially alcohol or tobacco, as this could magnify the health risks associated with these products (see “Special Focus: Cannabis, tobacco and alcohol” on page 44).
Vaping devices play an increasing role in cannabis consumption as they have with nicotine. We heard that the devices may offer a less-harmful alternative to smoking but that more evidence is needed about their risks and harms.
We also heard concerns regarding specific synthetic cannabinoids, e.g., “spice” – synthetic substances that share pharmacological similarity with THC but are not derived from the cannabis plant. These products are not considered part of the mandate of the Task Force: they have special risks and will remain controlled under the Controlled Drugs and Substances Act.
Advice to Ministers
The Task Force recommends that the federal government:
- Prohibit any product deemed to be “appealing to children,” including products that resemble or mimic familiar food items, are packaged to look like candy, or packaged in bright colours or with cartoon characters or other pictures or images that would appeal to children
- Require opaque, re-sealable packaging that is childproof or child-resistant to limit children’s access to any cannabis product
- Additionally, for edibles:
- Implement packaging with standardized, single servings, with a universal THC symbol
- Set a maximum amount of THC per serving and per product
- Prohibit mixed products, for example cannabis-infused alcoholic beverages or cannabis products with tobacco, nicotine or caffeine
- Require appropriate labelling on cannabis products, including:
- Text warning labels (e.g., “KEEP OUT OF REACH OF CHILDREN”)
- Levels of THC and CBD
- For edibles, labelling requirements that apply to food and beverage products
- Create a flexible legislative framework that could adapt to new evidence on specific product types, on the use of additives or sweeteners, or on specifying limits of THC or other components
THC potency
In our discussions about cannabis products, the Task Force heard a range of views about the risks associated with consuming cannabis products with high levels of THC and about the dangers associated with manufacturing some cannabis products, particularly those where highly combustible solvents, such as butane, and potentially toxic solvents such as naphtha, are used to extract THC.
Over the last few decades, changes in growing and production techniques have resulted in cannabis products with higher levels of THC. The “potency” (concentration) of THC is often expressed as a percentage of THC by weight of the substance (e.g., a flower, resin); the THC potency in dried cannabis (based on police seizures) has risen from an average of 3% in the 1980s to around 15% today. Some Canadian licensed medical cannabis producers are capable of growing cannabis with levels of THC higher than 30%. Resins extracted from the cannabis flower, which concentrate the cannabinoids, can have much higher potencies depending on how they are processed, ranging as high as 80% for solid concentrates known as “shatter.” Such high-potency concentrates are often ingested by heating a small amount on a hot surface, such as a nail, a method known as “dabbing.”
Despite studies showing that a typical user does not actually require large amounts of THC to experience the psychoactive effects of cannabis, the demand for, and availability of, products with higher levels of THC has persisted in jurisdictions that have legalized cannabis.
What we heard
Support for setting limits for THC content in cannabis products was strong among a range of stakeholders, particularly those with public health and health-care perspectives. Several also supported a ban on “high-potency products” (when defined, these were the highest-potency concentrates, such as wax and shatter).
These arguments were based on assumptions regarding higher risks of harm associated with higher potencies. Based on the current evidence, the higher the potency of THC, the lower the amount of a product required to achieve the desired effect, the higher the likelihood of developing dependence and the higher the likelihood – particularly with novice and inexperienced users – of an overdose.
Products containing higher levels of THC may trigger psychotic episodes in individuals at risk and may further increase the risk of harms to vulnerable populations, such as those with illness associated with psychosis.
Submissions advocating THC limits rarely specified what those limits should be. A few recommended a maximum of 15% THC potency in all products, though it is unclear why this level was chosen; there was also some acknowledgement that there is insufficient evidence to identify a “safe” potency limit. Nevertheless, many saw a THC limit as a necessary precaution.
There was also strong opposition from other respondents to the use of THC limits. A range of stakeholders agreed that, due to a lack of evidence, any such level would be arbitrary. Neither Colorado nor Washington has set limits on the amount of THC in concentrates.
Respondents to the online consultation asserted that users accustomed to high THC would either need to smoke a larger quantity of lower-potency cannabis to reach the desired effect, leading to higher smoking-related harms, or would simply turn to the illicit market for high-potency products.
The argument that banned products would continue to be available on the illicit market was one we heard several times. However, in this case, we were told that the stakes were considerably higher due to the significant risks of illicit production of high-potency concentrates. Illicit producers often use highly flammable solvents such as butane to extract cannabinoids from plants, an inherently dangerous process that can also leave carcinogenic residues on the end product. Product safety was also a concern, as the extraction process may also concentrate contaminants such as heavy metals and other impurities in addition to THC.
A number of alternate approaches were suggested to address the risks associated with potency:
- Clear labelling of THC levels on all products;
- Provision of consumer education about potency related risks;
- Low-risk use guidelines;
- Higher prices or taxes for higher potency products to shift consumers to products with lower potency; and
- Setting a higher minimum age, such as 25, for high-potency products.
There is also emerging evidence that the ratio of THC to CBD can play an important role in reducing some of the psychoactive effects of THC. Some roundtable participants believed that further research in this area could lead to innovations to modulate the effects of THC potency.
Considerations
The debate about whether to allow high-potency concentrates on the regulated market has similarities to our discussions on other cannabis-based products. One side emphasizes the risks of use of the products themselves, while the other highlights the consequences of allowing an illicit, unregulated market to continue.
While there may be risks of consuming high-potency concentrates, the dangers inherent in their production strongly suggest that they be included as a part of the regulated industry, subject to effective safety and quality-control restrictions. The harms associated with high THC potency remain a concern, and should be minimized. However, we do not believe that limiting THC content in concentrates is the most effective way to do so, based on current information. We agree that, due to a lack of evidence, any chosen threshold would be arbitrary and a challenge to enforce. Even the standard THC content of today’s dried cannabis is considered high by historical standards.
We suggest that variable tax rates or minimum prices linked to THC level (potency), similar to the pricing models used by several provinces and territories for beer, wine and spirits, should be applied to encourage consumers to purchase less-potent products.
We also recommend labelling all products with clear indications of their levels of THC and CBD, as well as appropriate health warnings. Such labelling must be based on mandatory laboratory testing that conforms to acceptable standards of accuracy.
We can expect that the evidence with respect to THC potency, including the effects of CBD to reduce the effects of THC, will continue to evolve. The system must have the means to implement further measures, including THC limits (and limits to other cannabinoids or their ratios), should future evidence warrant it.
Advice to Ministers
The Task Force recommends that the federal government:
- Provide regulatory oversight for cannabis concentrates to minimize the risks associated with illicit production
- Develop strategies to encourage consumption of less potent cannabis, including a price and tax scheme based on potency to discourage purchase of high-potency products
- Require all cannabis products to include labels identifying levels of THC and CBD
- Enable a flexible legislative framework that could adapt to new evidence to set rules for limits on THC or other components
- Develop and implement factual public education strategies to inform Canadians about the risks of problematic use and to provide guidance on lower-risk use
Tax and price
While government influence over price is often met with resistance in many industries, the risks associated with psychoactive substances can justify government intervention in this area. Used appropriately, price controls can discourage the use of cannabis and provide government with revenues to offset related costs. They are flexible tools, able to respond relatively quickly to emerging evidence. On the other hand, missteps on price can lead to unintended consequences: too low a price can inadvertently boost demand, while too high a price could shift consumers to seek lower-cost product in the illicit market.
Governments have a number of means to influence price, and therefore consumption, of a product. Many of these tools can be used together to control the price of a product:
- Fixed prices, i.e., specifying the price at which certain products must be sold;
- Minimum and/or maximum prices;
- Per unit taxes, i.e. a tax that charges a set amount per unit of a product;
- Sales tax, charged as a percentage of the sale price; and
- Limits on production amounts or on the number of producer licences.
What we heard
The Task Force heard about the need to strike a balance on price: higher prices will help to lower use, but prices that are too high will push consumers to the illicit market. Tobacco was often cited as an example of how price controls can achieve public health goals.
This balance could be adjusted strategically. A lower tax rate, initially, could help to avoid repeating the experience in Washington, where a high tax at the start of legalization, combined with a shortage of legal product, strengthened the existing illicit market. Taxes could be adjusted over time to reflect changes in market conditions.
We were cautioned that low prices could increase the consumption of cannabis overall. Sudden drops in price could result from a decrease in production costs for regulated cannabis, or from “predatory” pricing (i.e., pricing below one’s costs) meant to undercut competition. There is evidence that a drop in the price of cannabis can lead to new users, particularly among youth.
We heard that tax and price co-ordination between levels of government is critical. The federal, provincial and territorial governments have the authority to tax products such as cannabis, through either a unit tax or sales tax.
Most participants, including provincial and territorial officials with whom we met, agreed with the view that cannabis regulation should prioritize public health and safety, not revenues. However, there were opinions on how any resulting revenues should be allocated. Several stakeholders, including substance-use experts, law enforcement and municipalities, called on government to redirect revenues to support prevention and treatment programs for individuals with cannabis dependence. We also heard calls to direct a portion of tax revenues toward education programs, including targeted programs for youth, for Indigenous communities and for enforcement. Stakeholders also called for the allocation of tax revenues to support research on cannabis.
The Task Force also heard that we should:
- Establish a minimum price or tax based on potency levels, thereby driving consumers to less potent products;
- Encourage consistent prices and taxation levels across the country to avoid cross-border shopping. Some suggested considering additional taxes for tourists;
- Establish a Health and Safety Board to recommend and set prices; and
- Consider using economic analyses to learn how different costs, and availability of substances, impact consumption patterns.
Considerations
Putting public health concerns ahead of the generation of revenues is crucial to the success of a regulated cannabis market. Tax and price policies should therefore focus on achieving the Government’s public health and safety objectives. Taxes should be high enough to limit the growth of consumption, but low enough to compete effectively with the illicit market. Mechanisms such as a minimum price should be used to prevent predatory pricing, if necessary.
The federal government, in co-ordination with its provincial and territorial counterparts, should conduct the necessary economic analyses to determine a tax level that achieves the balance between public health objectives and reducing the illicit market. Municipalities and Indigenous national organizations and representatives should be included in discussions regarding the equitable allocation of revenues. Public health experts should also be included in this exercise to help ensure that the health burden is taken into account.
The Task Force also believes that building flexibility into the system will allow for adjustments based on new data. We also suggest that the federal government consider a THC potency-based minimum price or tax to shift consumers to lower-potency products (see “THC potency” in this chapter).
Advice to Ministers
The Task Force recommends that the federal government:
- Conduct the necessary economic analysis to establish an approach to tax and price that balances health protection with the goal of reducing the illicit market
- Work with provincial and territorial governments to determine a tax regime that includes equitable distribution of revenues
- Create a flexible system that can adapt tax and price approaches to changes within the marketplace
- Commit to using revenue from cannabis as a source of funding for https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistration, education, research and enforcement
- Design a tax scheme based on THC potency to discourage purchase of high-potency products
Public education
As we move away from prohibition, many stakeholders will turn to governments for information on how to assess the risks and harms of cannabis use and on how the regulation of cannabis will work. There is significant misinformation that must be addressed. Public opinion research shows that youth and some adults do not understand the risks of cannabis use. Typically they are either exaggerated (echoing the era of “reefer madness”) or understated (cannabis is benign).
What we heard
In the online consultation and in meetings with experts and officials, we heard that public education was critical to:
- Communicate information on the new system and its objectives;
- Help young people in particular understand the potential harms from cannabis use;
- Inform Canadians of the risks of impaired driving;
- Offset potential pro-consumption messages from industry and advocates, particularly those directed at children and vulnerable populations;
- Provide information on dependence and other risks of heavy consumption;
- Provide reliable information to customers at point of sale; and,
- Provide parents with information.
There was agreement that messaging about risks should be consistent across the country. Given the potential number of players delivering messages – including different levels of governments, non-governmental organizations and the private sector – a need for co-ordination was emphasized, often with the federal government in a leading role.
We heard that reaching youth with this messaging may be a challenge. Health experts and educators stressed that we need a new approach. Whether in schools or in national campaigns, education should be evidence-informed, credible, informative and respectful of youth judgment. We heard that youth should be involved in the design and content of education that is targeted at youth.
We heard that school programs should start at a young age. For adolescents, health experts recommended a focus on building competencies to help young people develop resiliency and critical thinking skills. Some jurisdictions are taking this approach in their schools already.
Education programs should not only be age-appropriate but also culturally appropriate. An Indigenous Elder who met with the Task Force called on the Government to work with Elders to develop culturally appropriate messaging on the risks of cannabis use for Indigenous youth.
In Washington and Colorado, funding for their respective education campaigns came from the states’ cannabis revenues. As a result, campaigns did not begin until two years after legalization. Officials from both states strongly advised starting educational campaigns as soon as possible.
Considerations
National campaigns and in-school programs are important components of an overall approach to public education on cannabis. Co-ordination between levels of government will be crucial. In meetings with the Task Force, provincial and territorial officials looked to leadership from the federal government on public education campaigns and health messaging.
Where strong provincial or territorial education programs on cannabis use exist, a federal public education campaign should enhance rather than replace existing programs and should learn from success stories.
Campaigns should: be evidence-informed; be relevant to, and respectful of, the target audience; and learn from successes and failures at home and elsewhere. A discussion specific to education campaigns for cannabis-impaired driving can be found in Chapter 4, Enforcing Public Safety and Protection.
Advice to Ministers
The Task Force recommends that the federal government:
- Implement as soon as possible an evidence-informed public education campaign, targeted at the general population but with an emphasis on youth, parents and vulnerable populations
- Co-ordinate messaging with provincial and territorial partners
- Adapt educational messages as evidence and understanding of health risks evolve, working with provincial and territorial partners
Prevention and treatment
While the regulation of cannabis aims to minimize harms for the general population, there are specific groups who may be negatively impacted, including youth with a history of early and frequent use, as well as adult heavy users and marginalized groups. Targeted measures will be needed to mitigate harms for these groups.
What we heard
In roundtable discussions, the Task Force often heard that there were certain groups for which education and other “population-level” measures were insufficient to reduce harms significantly. Most frequently, participants highlighted youth with a history of early and frequent use, or dependence. Other groups mentioned included adult heavy users, those with mental illness, people who are homeless and other marginalized groups.
We heard that reducing harms among these groups requires a public health strategy that includes special, targeted measures such as mental health strategies and investment in prevention and treatment programs for individuals and at-risk groups.
According to a number of health experts who work with youth, such approaches need to address individuals’ underlying issues, such as social isolation, problems at home or mental illness. They told us that some of the harms often attributed directly to cannabis use, such as dependence and lower academic achievement, can be better predicted by the existence of such life challenges.
Recent studies support this view. Analysis of results of the 2013 B.C. Adolescent Health Survey shows that youth who lived in challenging circumstances or who had experienced stressful life events, such as discrimination or physical or sexual abuse, were more likely to use cannabis frequently.
Such young, frequent users were more likely to feel disconnected from their school or community, to be dependent on alcohol or other substances, or to have attempted suicide. Often they lacked family support, positive relationships at school and other factors that reduce the risk of early or frequent cannabis use.
We also heard from law enforcement officials who observed similar issues in their work with “high-risk” individuals, including people who are homeless or mentally ill, and repeat offenders. We heard concerns that these individuals were at a greater risk of dependence and other harms.
There are many different approaches to prevention and treatment, and the Task Force heard some debate about their effectiveness. Ideally, targeted interventions should be evidence-based and should build resilience.
Programs should be tailored to meet the needs of different communities. For instance, Indigenous representatives told us that programs should be tailored to the unique circumstances of Indigenous communities.
Considerations
At the beginning of this chapter, we noted that a public health approach alone is insufficient to minimize harms experienced by vulnerable populations. Prevention efforts that address underlying causes of early, heavy and frequent use, especially among youth, are necessary to minimize harms.
Prevention and treatment programs often suffer from a lack of national co-ordination and sustained funding. Cannabis legalization offers an opportunity to redirect some of the new revenue stream to better support such programs.
Advice to Ministers
The Task Force recommends that:
- In the period leading up to legalization, and thereafter on an ongoing basis, governments invest effort and resources in developing, implementing and evaluating broad, holistic prevention strategies to address the underlying risk factors and determinants of problematic cannabis use, such as mental illness and social marginalization
- Governments commit to using revenue from cannabis regulation as a source of funding for prevention, education and treatment
Workplace safety
Drug and alcohol use or impairment in the workplace can pose a danger to everyone in the workplace, including the person who is impaired. This is particularly the case in “safety-sensitive” industries, such as transportation, health care and law enforcement, where symptoms related to impairment – reduced mobility, co-ordination, perception or awareness – can increase the risks of hazards, injuries and death.
The federal government and the provinces and territories each have their own occupational health and safety legislation and related regulations, which outline the general rights and responsibilities of employers and employees. At present there is no Canadian law permitting or regulating mandatory drug testing of employees. Court decisions, including those by the Supreme Court of Canada, provide some guidance and suggest that random drug and alcohol testing is not permitted except in certain circumstances. In addition, federal and provincial human rights commissions have policies explaining how drug and alcohol testing must not discriminate, including against those with disabilities and perceived disabilities. They suggest that drug testing in workplaces can only be used if it is to satisfy bona fide occupational requirements. Some private-sector companies have put drug testing policies in place, and the federal government has implemented testing programs for federal prisoners and military personnel.
Cannabis impairment in the workplace is not a new issue, but questions were raised about whether the legalization of cannabis might increase use and how that would affect workplace policies.
What we heard
The Task Force heard concerns from a range of experts and stakeholders about the impact of cannabis use in the workplace, particularly for people working in safety-sensitive positions, such as health-care workers, law enforcement personnel and employees in transportation, construction or resource extraction industries. We also heard about challenges associated with providing reasonable accommodation of employees who use cannabis for medical purposes or who may be dealing with dependence or other problematic use.
Employer groups called for more guidance from federal, provincial and territorial governments about appropriate workplace drug use and drug testing policies.
We also heard from health experts who looked at the issue from an employee perspective, noting the limited and uneven access to programs and services to support employees with dependence or other problematic substance use.
Considerations
The concerns expressed on workplace safety reinforce the urgent need for research to reliably determine when individuals are impaired. As we will see in Chapter 4, which addresses impaired driving, the ability to determine impairment with cannabis – through technology or specialized training – is not as advanced as our ability to measure the relationship between consumption and impairment with alcohol.
Should new evidence on cannabis impairment merit changes in workplace safety policies, the federal government should work closely with the provincial and territorial governments, given their shared roles in the occupational health and safety system, to consider and respond to the implications of this evidence.
Advice to Ministers
The Task Force recommends that the federal government:
- Facilitate and monitor ongoing research on cannabis and impairment, considering implications for occupational health and safety policies
- Work with existing federal, provincial and territorial bodies to better understand potential occupational health and safety issues related to cannabis impairment
- Work with provinces, territories, employers and labour representatives to facilitate the development of workplace impairment policies
Special Focus: Cannabis, alcohol and tobacco
A common concern among stakeholders was the impact of cannabis use on the use of alcohol and tobacco, and vice versa. We heard that using these products in combination, or even selling them in the same location, could magnify the health risks associated with each and have other negative implications. It was even suggested that minimizing co-use of cannabis and alcohol or tobacco could be a specific health protection aim of cannabis policy.
The harms of alcohol and tobacco are well established. According to the Chief Public Health Officer’s Report on the State of Public Health in Canada (2015), almost 80 percent of Canadians consume alcohol; in 2013, more than 7.4 million Canadians drank enough to be at risk for immediate injury and harm or for chronic health effects, such as liver cirrhosis and cancer. Tobacco-related illness is responsible for 37,000 deaths in Canada each year and results in $4.4 billion of direct health-care costs.
We heard from many stakeholders that co-use of cannabis with alcohol should be discouraged, given the implications for public health and safety. Research shows that the simultaneous use of alcohol and cannabis significantly increases levels of THC in the blood. This has implications for behaviour while intoxicated, and particularly for impaired driving (see Chapter 4). In addition, having cannabis and alcohol sold in the same location was seen by many as encouraging co-use (see Chapter 3).
We also heard that co-use of cannabis and tobacco products could undermine the progress achieved over the last few decades on reducing smoking. The Canadian Community Health Survey indicates that the rate of tobacco smoking among cannabis users is more than double that of those who do not use cannabis. This leads to concerns, particularly from anti-tobacco organizations, that increased cannabis use, or co-sale with tobacco, could lead to an increase in tobacco use and nicotine dependence.
The Task Force agrees that minimizing the harms of cannabis use also means taking steps to avoid co-use with alcohol and tobacco. This view is reflected in recommendations in Chapters 2, 3 and 4 of this report.
Chapter 3: Establishing a Safe and Responsible Supply Chain
Introduction
As noted in Chapter 1, two of the major themes that formed the basis of the Task Force’s discussions and consultations were “establishing a safe and responsible production system” and “designing an appropriate distribution system.” We noted during Task Force consultations that conversations surrounding these two themes coalesced into an integrated discussion about the entire supply chain, encompassing production (commercial and personal cultivation), distribution and retail. This chapter will mirror that shift and discuss how to regulate the supply chain in its entirety.
Decisions on production, distribution and retail have clear implications for businesses hoping to enter the cannabis industry, including how to ensure a diversity of participants. It is apparent that there is significant interest and speculation about the potential for new revenues generated by this industry.
Supply chain management also has significant implications for consumers and communities. Price, product quality and accessibility can all be affected, depending upon what route the Government chooses to take.
Notwithstanding this interest and the far-reaching implications of decisions made regarding the nature and scope of the new industry, the Government’s principal interest should be to establish an efficient, accountable and transparent system for regulatory oversight of the supply chain, emphasizing the protection of health and safety and reducing diversion to the illicit market.
Production
Cannabis production ranges from the cultivation and harvest of the plant material, and its subsequent preparation, to the manufacture of products using cannabis as a raw material including concentrates and other derivatives.
What we heard
Throughout our consultations, there was support for commercial production of cannabis being left in the hands of the private sector. The vast majority of respondents to the online consultation expressed a preference for a competitive private-sector production model, noting that this would allow for a greater variety and diversity of products with fair pricing. However, some organizations believed that a government monopoly would be the best approach to control and regulate the production of cannabis, noting that this model was best placed for controlling use, preventing diversion, minimizing advertising and helping to control pricing. In both models, respondents indicated an expectation that the federal government would continue to regulate production. Most respondents thought that cannabis distribution and retail should be regulated by the provinces and territories.
Having the federal government regulate cannabis production was seen as essential for a variety of reasons; such as to ensure that consumers in all regions of the country have access to quality-controlled products that are free from harmful pesticides, fungi and bacteria, heavy metals and other harmful substances. The federal government was seen as being well-placed to establish and oversee a national regulatory system of quality control, given that such a system is already in place for the production of cannabis for medical purposes.
Many noted that the current federal system of cannabis for medical purposes could be used as a starting point for a new national system for legalized and regulated cannabis. Under the current system, companies seek licences from Health Canada to produce and distribute cannabis for medical purposes and must comply with a set of strict rules to meet safety and quality standards and security provisions.
Many of those standards were seen as applicable when contemplating production in the new legal system in order to protect public health and safety. As noted in Chapter 2, the processing of extracts is one area where stakeholders saw regulation as key to mitigating significant potential harms.
Some stakeholders expressed concern that, under a regulated, non-medical cannabis framework, the current security requirements would be unnecessarily strict, such as the requirement to keep security video recordings for two years. Some expressed concern that the cost of compliance with such security regulations might suppress competition in the marketplace and could potentially shut out smaller, new producers in favour of larger companies or conglomerates that could better afford these measures.
We heard from representatives of those currently operating in the illicit cannabis economy who differentiated themselves from organized criminal enterprises. They expressed a keen desire to legitimize their businesses by transitioning into the legal market but were also concerned that they would be excluded by design, or due to their current involvement in the illicit market. They, and others, made strong calls for a diverse marketplace in which barriers to the participation of smaller producers (sometimes referred to as “craft” or “artisanal”) and not-for-profit entities are kept to a minimum. Likewise, in order for these individuals or businesses to be eligible to qualify for government-issued licences, they asked that some allowance be made for individuals who may have criminal histories with cannabis.
Some stakeholders questioned the current requirement for licensed producers to grow cannabis indoors. They expressed concern that prohibiting outdoor cultivation would create a financial barrier for smaller enterprises to enter the market. We also heard that indoor growing does not promote environmental stewardship, due to significant electrical and water costs.
The cannabis for medical purposes system requires the testing of products for impurities such as heavy metals and microbial contaminants through approved laboratories. Many noted that this requirement needed to be extended to the new system. We also heard that product labels need to accurately and reliably reflect THC and CBD potency, allowing consumers to make informed decisions.
Industrial hemp
Varieties of the cannabis plant known as hemp have long been cultivated for use in commercial and industrial applications such as construction materials, rope and clothing. In 1998, through the Industrial Hemp Regulations (IHR), the Government provided for the creation of an industrial hemp industry in Canada. The IHR set out a licensing and permit scheme through which industrial hemp producers are able to cultivate hemp, defined as cannabis plants that have less than 0.3% THC. Currently, producers are permitted to use only the seeds, grains and fibres from the hemp plant.
We heard from members of the hemp industry that, although low in THC, hemp can contain high levels of non-psychoactive CBD. Despite this, the rules around growing hemp have mainly reflected concerns that hemp fields could be a cover for growing high-THC cannabis. Hemp producers face burdensome requirements, including the need for repeated field testing to ensure that the THC threshold is not exceeded, the requirement to re-apply for a licence every year and a requirement to submit maps of every field where industrial hemp is grown. In addition, it is unlikely that producers will grow high-THC cannabis since the growing environment for hemp is not conducive for flowering varieties of cannabis that contain higher concentrations of THC.
Further, the IHR require the destruction of plant material for which there is no authorized use, including parts of the plant that are high in CBD. We have heard that increasing interest in the therapeutic value of CBD presents an economic opportunity for hemp producers, as hemp may be a rich source of CBD for therapeutic products.
Considerations
The Task Force agrees that the new regulatory framework should ensure that products meet rigorous safety and quality standards in order to protect public health and safety. For example, only approved fertilizers and pesticides should be allowed; potentially hazardous moulds should not be present; product-specific THC and CBD potencies, including serving sizes, should be established and verified; and potentially hazardous extraction processes should be undertaken with the proper safety measures in place. Given the federal government’s experience with regulating the medical cannabis system, commercial production should continue to be regulated by the federal government, and should include appropriate licensing fees to recover the costs of https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistration.
This will require sufficient laboratory testing capacity to ensure that the products manufactured meet specific quality standards and that the stated potency for specific products is accurate.
The framework should draw from the good production practices already established for licensed producers of cannabis for medical purposes, including the use of approved pesticides, testing for solvent residues, testing for THC and CBD levels, and sanitation of premises and equipment.
At the same time, the framework should reconsider existing security requirements that are in place under the Access to Cannabis for Medical Purposes Regulations. We acknowledge that security requirements should not be so strict that they are prohibitively expensive or difficult to implement, thus creating unnecessary barriers to entry into the regulated marketplace.
Given the significant interest that exists among a diversity of citizens, industry sectors and investors to participate in this new regulated market, it will be necessary to have an effective, accountable and efficient regulatory program in place at the time of implementation.
In developing the new system for licensing cannabis producers, it will be important to understand the size and nature of the new regulated market and to determine whether controls to align supply with likely demand are required to avoid situations of oversupply, which could lead to negative outcomes. Some congruence between the amount of cannabis required to meet the demands of the Canadian market and the total quantity allowed for production could serve to minimize risks, at least in the early years of implementation as the marketplace develops. For example, this could be done by limiting the number of production licences issued or the total amount that any one producer is allowed to supply.
There are several advantages to using production controls in the early period of implementation, including:
- Encouraging market diversity by creating a space for smaller-scale production through graduated licensing and fee structures, and preventing the development of monopolies or large conglomerates;
- Preventing an oversaturation of the market, potentially contributing to over-consumption or problematic consumption;
- Controlling cannabis prices by increasing or decreasing the number of production licences issued or by imposing limits on the size of facilities; and
- Creating an https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistratively efficient regulatory program that is resourced appropriately.
However, limiting the number of production facilities or the size of those facilities must be balanced against the possible miscalculation of demand that would create opportunities for illicit producers to fill the void.
Diversion can also be addressed through a requirement that all businesses in the cannabis supply chain implement a seed-to-sale tracking system, similar to that used in the U.S. states that have legalized cannabis. Such a system would monitor the movement of cannabis plants and resulting products throughout the supply chain – from production to distribution to final sale. Such a system has several other benefits, including the ability to trace products in the event of a recall, and can be helpful for producers in the management of their inventory.
In order to limit the environmental impact of the cannabis industry, outdoor production should be permitted with adequate security requirements. Encouraging responsible environmental practices through less reliance on indoor lighting, irrigation networks and environmental controls (i.e., heating and cooling, humidity controls) can contribute to substantially reducing the environmental footprint of cannabis production facilities. Outdoor growing could also help reduce costs and enable entry for smaller “craft” producers.
While the new legislation will apply to cannabis, including industrial hemp, we believe a lighter regime should be designed to regulate the industrial hemp industry. With respect to CBD and other compounds derived from hemp or other sources, each substance should be reviewed and regulated depending on its risks.
Advice to Ministers
The Task Force recommends that the federal government:
- Regulate the production of cannabis and its derivatives (e.g., edibles, concentrates) at the federal level, drawing on the good production practices of the current cannabis for medical purposes system
- Use licensing and production controls to encourage a diverse, competitive market that also includes small producers
- Implement a seed-to-sale tracking system to prevent diversion and enable product recalls
- Promote environmental stewardship by implementing measures such as permitting outdoor production, with appropriate security measures
- Implement a fee structure to recover https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative costs (e.g., licensing)
- Regulate CBD and other compounds derived from hemp or from other sources
Distribution
A well-functioning distribution system – where the chain of custody is well-controlled – is critical to the overall success of the new regime.
What we heard
As noted above, while the federal government was generally seen as best placed to regulate the production of cannabis, most respondents believed that the provinces and territories should be the principal regulators of wholesale distribution. Indeed, most jurisdictions noted during our consultations that they had well-established and sophisticated government alcohol distribution networks that provided a secure and reliable means to distribute product. It was noted that these systems, especially the https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative systems and other controls already in place, could be leveraged to distribute cannabis and be tailored to the specific needs of each jurisdiction.
Considerations
Implementing a government monopoly on wholesale distribution has been widely supported. It has proven effective with alcohol as a means to prevent diversion and to maintain controls over supply.
Advice to Ministers
The Task Force recommends that the wholesale distribution of cannabis be regulated by provinces and territories.
Retail
Under a regulated system, consumers should be able to access cannabis in a safe manner that minimizes potential risks to consumers and communities and reduces the involvement of the illicit market.
What we heard
The Task Force heard mixed views on the type of retail outlets that should be permitted. Some advocated for a centralized, government monopoly akin to how most provinces and territories manage alcohol sales while others expressed a preference for a private-enterprise model with cannabis-specific storefronts (e.g., dispensaries) or with those for whom profit is not their principal motive (e.g., compassion clubs). Regardless of the model, participants were generally of the view that there should be some sort of storefront retail market, but they also noted concerns regarding the unchecked proliferation of unregulated dispensaries as they exist today.
There was also support for extending the current system of mail-order purchasing of cannabis. This was especially important to those from rural and remote communities where a physical store might not be viable.
We also heard that the mail-order system was insufficient for the broader non-medical cannabis market. Many expressed a preference for engaging more directly with knowledgeable staff and with the products themselves before making purchases. Thus, support for the private-enterprise model was widespread among respondents to the online questionnaire and among experts consulted during our roundtable sessions. This model of retail sales was cited often as a means of ensuring access and encouraging a competitive, open market on pricing which might then be able to compete with, and help limit the use of, the illicit market.
Conversely, some provinces and territories and public health experts advocated for government monopolies. They cited concerns that the private-enterprise model could oversupply the market if storefronts were allowed to proliferate unchecked. This could lead to overconsumption and overuse by at-risk populations. Government-controlled outlets might be more likely to demand proof of age, refuse sales to underage or apparently impaired customers, sell only products supplied by licensed producers and comply with other federal regulatory limits.
Regardless of the model chosen, there was strong support for ensuring employees would be well trained to inform consumers of responsible use and the risks of use/overuse, and to provide information on the different product types available to allow consumers to make informed choices. This was believed to be more likely in a retail environment that favoured single-purpose or dedicated cannabis sales. Vendor training was seen as a way to provide some consistency of the information provided to consumers.
Additionally, the Task Force heard strong support for prohibiting the co-location of cannabis sales with either alcohol or tobacco. Given the wide use and availability of liquor stores, concerns were raised about product promotion and exposing a larger population to cannabis products should sales be co-located, as well as the impact on cannabis consumers who are trying to avoid alcohol. Many also noted that this approach could help mitigate co-use, given what we heard about the risks of co-use on health and, with alcohol, the exponential effect on impairment. In all of the U.S. states that have legalized cannabis, there is a ban on the co-location of sales of cannabis and alcohol.
There was strong support for measures to control the density and location of retail stores. These measures prohibit storefronts from being located near schools, community centres and other public institutions. However, concerns were raised about the “downloading” of these regulatory responsibilities and costs to municipalities.
Considerations
Retail sales should be regulated by provinces and territories in close collaboration with municipalities. As with production, appropriate licensing fees should be established to recover the costs of https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistration. The Task Force sees the merits of both a government-run model and a private-enterprise model. Either model could achieve the goals of protecting public health and safety, reducing the illicit market and controlling youth access. Ultimately, the Task Force believes that this decision rests with individual jurisdictions, but regardless of the model chosen, we believe that certain standards should be put in place and followed.
In their report Public Health Perspectives on Cannabis Policy and Regulation, Chief Medical Officers of Health note several public health concerns with the co-location of sales. Of particular concern is that, given the high rate of alcohol use by the adult population (over 80% of Canadians consume alcohol) compared to the relatively small usage rate of cannabis (approximately 11% of adults have consumed cannabis in the past year), there is a significant risk of cannabis and cannabis advertising being introduced to a large number of Canadians who might not otherwise use cannabis. In Ontario, for example, there are more than 137 million individual in-store transactions at the 654 Liquor Control Board of Ontario (LCBO) stores annually Footnote5. Similarly, in BC there are more than 36 million individual annual customer visits to the 199 BC Liquor Stores Footnote6. The potential for increasing rates of use and co-use run counter to the public health objectives of harm reduction and prevention.
In addition, co-location of sales might signify to some that co-use of cannabis and alcohol or tobacco is condoned or encouraged. We heard repeatedly about the significant risks of co-use to public health and safety, especially with respect to driving (see the “Impaired Driving” section in Chapter 4), and that governments must do whatever they can to prevent it. While there is little research to confirm that there is a direct correlation between co-location and co-use, a precautionary approach, combined with the example of how other governments have dealt with this issue, supports reducing possible risks by banning co-location of sales wherever possible.
Jurisdictions should avoid and strongly discourage the co-location of retail cannabis and alcohol or tobacco sales wherever possible. We acknowledge the challenges of smaller and remote communities that may not have the flexibility to accommodate dedicated, separate retail locations. Should separate retail locations not be feasible everywhere, safeguards to mitigate potential harms should be put in place to discourage co-use and mitigate the other concerns that have been raised. These should include training staff and using clear signage to educate and inform customers of the risks of co-use, banning cross promotion and stocking alcohol/tobacco and cannabis in physically separated spaces.
In order to control access and curb overconsumption, provinces, territories and municipalities should consider using legislation and bylaws to prevent the proliferation of storefronts, including stores selling cannabis or cannabis paraphernalia, and to ensure locations are an acceptable distance away from schools, community centres, public parks, etc.
Retail outlets should be staffed with knowledgeable employees who have been trained through a formal training program, which will need to be developed. The training should ensure that staff are capable of:
- Providing accurate information and advice about the products being sold, and their potential risks and harms of use;
- Enforcing the minimum-age restriction and helping prevent youth access;
- Helping control overconsumption by informing consumers about appropriate and responsible use, and preventing sales to intoxicated consumers; and
- Informing tourists who purchase cannabis of their rights and obligations, especially with respect to not attempting to take cannabis across international borders.
Consideration should also be given to ensuring that online retail sales have appropriate consumer safeguards.
To accommodate those who may not have access to storefronts (e.g., small communities, rural and remote locations, mobility-challenged individuals) a direct-to-consumer mail-order system for non-medical cannabis should be considered. This will require appropriate provincial and territorial oversight.
Advice to Ministers
The Task Force recommends that retail sales of cannabis be regulated by provinces and territories in close collaboration with municipalities.
The Task Force further recommends that the retail environment include:
- No co-location of alcohol or tobacco and cannabis sales, wherever possible. When co-location cannot be avoided, appropriate safeguards must be put in place
- Limits on the density and location of storefronts, including appropriate distance from schools, community centres, public parks, etc.
- Dedicated storefronts with well-trained, knowledgeable staff
- Access via a direct-to-consumer mail-order system
Personal cultivation
Apart from the commercial production, distribution and retail supply chain, personal cultivation provides a potential alternative means for consumers to access cannabis.
What we heard
Few topics of discussion generated stronger views than the question of whether to allow Canadians to grow cannabis in their homes for their own consumption. There are strong arguments both for and against allowing the personal cultivation of cannabis, shaped by Canadians’ experience with home cultivation of cannabis over recent decades.
On the one hand, we heard compelling arguments in favour of prohibiting personal cultivation, notably in homes, because of the health and safety risks it can pose, the challenges associated with oversight and the potential ease with which it can be diverted to supply illicit markets. We also heard compelling arguments in favour of allowing personal cultivation, premised on the belief that personal cultivation can be done safely and responsibly.
Arguments against allowing for personal cultivation are largely shaped by current experience with large-scale grow-ops operating in a clandestine fashion in communities across Canada. We heard from law enforcement, municipal officials, landlords, neighbours and parents of uncontrolled, intrusive and dangerous commercial-scale operations that damage properties and threaten the safety of neighbourhoods. The concerns were numerous: risks associated with mould when large-scale growing occurs in buildings not designed or properly equipped to do so; improper electrical installation and associated fire hazards; unchecked use of pesticides and fertilizers; and break-ins and thefts – all of which result in dangers to neighbouring residences and first responders. Instances of explosions resulting from attempts to manufacture concentrates in a home-cultivation setting were also referenced.
These concerns were echoed when we visited Colorado. For example, law enforcement officials in Colorado described their recent experiences where global criminal organizations have established themselves in their state in order to produce cannabis for illicit markets.
Proponents of personal cultivation argue that, once a regulated, legal market for cannabis is established, the demand for illicitly produced cannabis should significantly decline and, over time, disappear. It follows that, as demand for illicit cannabis declines, so too will the number of large, commercial-scale illicit grow-ops and the risks they pose to public health and safety.
Proponents of personal cultivation further argue that, similar to alcohol, the majority of consumers will purchase from the legal market and few will choose to cultivate their own cannabis. Those who choose to cultivate will largely be law-abiding adults who grow a limited number of plants in a safe and responsible manner for their personal use (again, similar to the current circumstance with home brewing of alcohol).
From responses to the online consultation, there was widespread support for the inclusion of personal cultivation in a regulated regime. In fact, 92% of those who responded to the question were in favour of personal cultivation. Proponents cited a variety of arguments for allowing personal cultivation, including cost, personal preferences and access for those in rural and remote communities.
The law enforcement community has indicated a preference for a complete prohibition on personal cultivation. However, they also acknowledge the practical difficulties of trying to enforce a complete ban on cultivation for personal use.
Many who argued in favour of the personal cultivation of cannabis agreed that rules are required, such as prohibiting any unlicensed commercial production and sale, and preventing minors from accessing cannabis.
The Task Force heard from other jurisdictions which have allowed small-scale, own-use cultivation in tandem with a range of measures to help mitigate associated risks. The table below outlines how others have dealt with personal cultivation.
| Washington | District of Columbia | Oregon | Colorado | Alaska | |
|---|---|---|---|---|---|
| Personal cultivation | Not permitted (remains illegal) | Up to 6 plants — up to 3 mature — per adult (Maximum of 12 plants per residence — 6 being mature — in a single house or rental unit) | Up to 4 plants per residence(regardless of the number of adults residing at the residence) | Up to 6 plants — up to 3 mature — per adult, in a fully enclosed, locked space(Maximum of 12 plants per residence, regardless of the number of adults living in the residence) | Up to 6 plants — maximum of 3 mature — per adult |
| Location | N/A | Indoor only — within the interior of a house or rental unit | Indoor and outdoor permitted | Indoor and outdoor permitted | Indoor and outdoor permitted |
Considerations
It is currently legal to grow and produce tobacco for personal use in Canada (up to 15 kg of tobacco or cigars), just as it is legal to produce wine or beer at a residence for personal use. Wine-making, home brewing of beer and curing personally grown tobacco is undertaken primarily by advocates and connoisseurs in the post-Prohibition era. It is assumed that, over time, personally cultivated cannabis will follow the same course.
The experiences of Colorado and Washington with respect to the potential diversion of personally cultivated cannabis must be taken in context. In the United States, cannabis for non-medical purposes is illegal federally and in all but nine U.S. jurisdictions (eight states and Washington, D.C.). This contributes to demand from states where cannabis remains illegal. By enabling legal access to cannabis on a national level in Canada, it is anticipated that the demand for illicitly produced cannabis will diminish over time.
Small-scale cultivation of cannabis in the home is not without risks. Of particular concern is the exposure of children to cannabis. As a result, safeguards are important. Measures that have been adopted in other jurisdictions include lockable spaces for indoor production, securely fenced areas for outdoor production and ensuring plants are not visible from the street or from adjacent dwellings.
With a clear understanding of the risks associated with personal cultivation, the following safeguards would create a reasonable framework for enabling small-scale cultivation of cannabis for personal use:
- Set clear limits on the scale of cultivation permitted (maximum of four plants per residence), with a maximum height limit (100 cm);
- Prohibit unlicensed sale (although some degree of sharing among friends and relatives is inevitable);
- Prohibit the manufacture of concentrates in homes using volatile solvents and chemicals;
- Establish guidelines to ensure cultivation is in spaces not visible or accessible to children;
- Encourage local authorities to establish their own oversight and approval frameworks, such as requiring individuals to notify local authorities if they are undertaking personal cultivation;
- Regulate the market to enable a legal source for starting materials (e.g., seeds, seedlings, plant cuttings).
Advice to Ministers
The Task Force recommends allowing personal cultivation of cannabis for non-medical purposes with the following conditions:
- A limit of four plants per residence
- A maximum height limit of 100 cm on the plants
- A prohibition on dangerous manufacturing processes
- Reasonable security measures to prevent theft and youth access
- Oversight and approval by local authorities
Chapter 4: Enforcing Public Safety and Protection
Introduction
The Task Force heard the need for clear, enforceable rules to ensure all Canadians and law enforcement agencies understand what is permitted (and under what conditions) and what continues to be prohibited in the new legal regime. We also heard that penalties for contravening the rules need to be proportional to the contravention and that the criminal justice system should only be employed where necessary.
Currently, the impact of being arrested and convicted for simple cannabis possession offences has serious ramifications. The stigma of arrest, and the possibility of having a criminal record, are life-long consequences.
Illegal activities
What we heard
Notwithstanding the Government’s objective to eliminate the illegal market, law enforcement cautioned us that even a well-regulated, accessible and competitive industry will not completely eliminate illicit activity related to cannabis. While most consumers will prefer to purchase cannabis from a reliable, regulated, legal source, the Government should expect that there will continue to be attempts to operate outside of the legal regime. In moving to enact this new regime with clear rules, criminal penalties should be reserved for the most serious offences. There was strong support for addressing infractions by regulated parties – producers, distributors and retailers – within a regulatory framework, except where such activity threatened public safety.
A key area of concern was trafficking of cannabis. Many suggested that illicit production, trafficking, possession for the purposes of trafficking, possession for the purposes of export, and the import/export of cannabis outside of the new legal framework should continue to be prosecuted through criminal law. And, the focus should remain on illicit activities for commercial gain, not “social sharing”.
Given the additional risks associated with early and frequent use of cannabis, there was widespread agreement that criminal sanctions should be maintained with respect to providing cannabis to youth. Some respondents questioned whether criminal penalties would be appropriate in all situations, such as a family member providing a small amount of cannabis to youth for consumption at home (provincial and territorial alcohol schemes generally provide exemptions for such situations).
Overwhelmingly, respondents took the view that the criminalization of youth should be avoided. Most felt that criminal sanctions should be focused on adults who provide cannabis to youth, not on the youth themselves.
There was general agreement that non-criminal approaches should be implemented to discourage youth from possessing or consuming cannabis. Measures such as peer-organized support programs, community service and attendance at education courses were seen as effective means of giving youth the tools to assess, and better understand, the harms of their cannabis use. Some respondents raised concerns with the ticketing of youth, as this might lead to inequitable situations for youth living in challenging socio-economic circumstances.
Considerations
We recognize that organized crime is involved in the illicit cannabis markets, domestically and internationally. A robust and regulated production, distribution and retail network that meets demand in the domestic market will help curb the illicit market and help identify those who operate outside the legal market.
The sale of cannabis to minors should remain a criminal offence, as one of the primary objectives of legalization is to keep cannabis out of the hands of youth. Consideration should be given to excluding certain situations from criminal penalties, such as when a parent provides a small amount to a teenager to use while in a private setting.
We are mindful of the negative consequences that involvement in the criminal justice system can have for youth, especially disadvantaged or marginalized youth, and believe that this should be avoided to the extent possible. To that end, we do not believe that simple possession of cannabis by youth should be a criminal offence (apart from the limits on personal possession, discussed below). When youth engage in activities that are defined as criminal offences under the new framework, the discretion and flexibility available in the criminal justice system, in particular under the Youth Criminal Justice Act, should be used constructively to minimize these negative consequences.
Regulatory sanctions should be proportionate to the contravention and include a range of enforcement options. For example, monetary penalties could be used to encourage licensed businesses to comply with the rules around packaging requirements for edible products, labelling on products and mandatory testing of products. Repeat violations or product safety concerns could be treated more severely (i.e., licence revocation or mandatory product recalls). In serious cases (e.g., trafficking to foreign markets), the ability to lay criminal charges must be retained. The majority of Task Force members believe that criminal offences should also be retained for other serious offences such as illicit production and trafficking.
Although some criminal offences relating to cannabis should continue to exist, they do not have to be in the Controlled Drugs and Substances Act. During our consultations, a few individuals and organizations raised questions about the form that the new legal framework would take and, in particular, whether cannabis should be removed from the scope of the CDSA. Ultimately these will be matters for the Government to determine, as our discussions have focused on the substance of the new framework rather than its form. However, the Task Force sees several advantages to the creation of new federal legislation dealing with cannabis.
This new legislation could bring together, in a single coherent set of provisions and regulations, the full range of issues relating to cannabis, including the production and marketing of cannabis products, their medical uses and regulation of the hemp industry. It could contain https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative sanctions to enforce the regulatory regime as well as a set of criminal offences. If cannabis were to remain under the CDSA, extensive amendments would be required to give effect to our recommendations. Separate legislation dedicated to cannabis would recognize a new beginning and provide a clear framework for industry and members of the public.
Advice to Ministers
The Task Force recommends that the federal government:
- Implement a set of clear, proportional and enforceable penalties that seek to limit criminal prosecution for less serious offences. Criminal offences should be maintained for:
- Illicit production, trafficking, possession for the purposes of trafficking, possession for the purposes of export, and import/export
- Trafficking to youth
- Create exclusions for “social sharing”
- Implement https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative penalties (with flexibility to enforce more serious penalties) for contraventions of licensing rules on production, distribution and sale
- Consider creating distinct legislation – a “Cannabis Control Act” – to house all the provisions, regulations, sanctions and offences relating to cannabis
Personal possession
Under a regulated system, adults who choose to use cannabis should be able to carry it with them to use responsibly. To some people, there should be no limits on the ability to carry a legal substance while, to others, possession of large amounts of cannabis could indicate intent to traffic. Deciding whether to recommend a limit on personal possession was a major issue for the Task Force.
What we heard
The Task Force heard different points of view on whether there should be a limit on the amount of cannabis an individual could have in their possession or on their person at any given time.
Many law enforcement officials argued in favour of personal possession limits, suggesting that such limits could be used as a tool to identify, investigate and prosecute individuals who may be engaging in illicit activity. This argument gains support from the fact that all other jurisdictions that have legalized cannabis have established a personal possession limit (see Table 2).
| Uruguay | Washington | District of Columbia | Oregon | Colorado | Alaska | |
|---|---|---|---|---|---|---|
| Personal possession limits | 40 grams per month.Customers must register at point of sale (pharmacy); the information is collected in a federal database | A combined maximum of:
|
2 oz. or less | 8 oz.1 oz. can be carried on the person | 1 oz. or its equivalent | 1 oz. |
| Total | 40 grams per month | 28.5 grams dried (or the equivalent) | 57 grams | 226 grams (only 28.5 g can be carried on the person) | 28.5 grams | 28.5 grams |
While quantity alone is not indicative of trafficking, it can be an indicator and, in conjunction with other indicators (e.g., large amounts of cash on hand, small individual packages of cannabis), could help in determining whether to lay trafficking charges. The focus of investigative efforts should be on whether someone has the intent to traffic and not exclusively on the amount they possess. We were reminded that someone with an amount of cannabis under the prescribed limit could also be guilty of trafficking.
The Task Force also heard from a number of respondents who believe that a personal possession limit is unnecessary. They argue that there is no possession limit for legally purchased alcohol and tobacco, and that a personal possession limit would be impractical to enforce.
Considerations
All jurisdictions that have legalized cannabis for non-medical use have instituted a possession limit. The majority of the Task Force agrees that instituting a similar limit in Canada would be a reasonable precaution that may also provide clarity to assist law enforcement efforts. The amount of non-medical cannabis that individuals are permitted to carry on their person in a public place should be limited to 30 grams. A corresponding limit should be imposed on the amount that can be sold to an individual at one time.
As in other jurisdictions, this limit would apply to dried cannabis. An equivalent possession and sales limit for non-dried forms of cannabis will need to be developed.
Offences with respect to exceeding the limit should be dealt with through graduated https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative penalties (e.g., tickets, seizures, fines) except where there is evidence of intent to traffic.
Advice to Ministers
The Task Force recommends that:
- A limit of 30 grams be implemented for the personal possession of non-medical dried cannabis in public
- A corresponding sales limit be implemented for dried cannabis
- Equivalent possession and sales limits for non-dried forms of cannabis be developed
Place of use
An important consideration in a regulated cannabis regime is how and where adult users may responsibly use cannabis without affecting the health and well-being of others.
What we heard
Traditionally, cannabis has been a smoked product. We heard concern about public use of cannabis and the general nuisance of second-hand smoke. We heard repeatedly that rules on place of use should align with current restrictions on smoking tobacco – clear recognition that second-hand smoke, regardless of the source, is a health hazard and viewed as an imposition in modern society. There is also concern that allowing the smoking or the increasingly popular vaping of cannabis in public spaces could potentially contribute to the “renormalization” of tobacco use and could undermine progress made to date on lowering tobacco consumption rates.
There was some discussion about permitting cannabis use in designated public spaces, such as cannabis lounges, tasting rooms or social clubs. Some expressed concern with the lack of private spaces available to certain demographics (e.g., renters, homeless individuals).
Considerations
The Task Force agrees with the widespread view that current restrictions on public smoking be extended to include the public smoking of cannabis. We do not want to see cannabis use contribute to a resurgence of tobacco smoking, nor do we want second-hand smoke (tobacco or cannabis) to affect the health of Canadians.
Many jurisdictions have taken steps to ban public use of vaping devices. While we acknowledge the ongoing debate over the merits of vaping products compared with smoking, we also recognize the jurisdiction of provinces, territories and municipalities in this regard.
Advice to Ministers
The Task Force recommends that jurisdictions extend the current restrictions on public smoking of tobacco products to the smoking of cannabis products and to cannabis vaping products.
The Task Force further recommends that jurisdictions be able to permit dedicated places to consume cannabis such as cannabis lounges and tasting rooms if they wish to do so, with no federal prohibition. Safeguards to prevent the co-consumption with alcohol, prevent underage use, and protect health and safety should be implemented.
Impaired driving
Throughout our consultations, cannabis-impaired driving generated a great deal of concern and discussion. It is clear that there is heightened anxiety that legalization may lead to increased dangers on the road, putting the safety of Canadians at risk. Yet there is uncertainty as to the most appropriate course of action, owing to the lack of scientific evidence on some aspects and a lack of means to reliably assess impairment at the roadside.
What we heard
Law enforcement and other experts made it clear that cannabis-impaired driving is not a new challenge. It is a criminal offence that exists today and is a challenge that must be addressed, irrespective of how or when the Government legalizes cannabis. It is also an issue that transcends cannabis: impairment more generally, whether from cannabis, alcohol, prescription or illegal drugs, fatigue or other factors, is a significant road safety concern.
It is clear that cannabis impairs psychomotor skills and judgment. While there is a link between cannabis use and decreased driving performance and increased crash risk, several considerations were noted:
- Cannabis-impaired driving is more complex to study than alcohol-impaired driving;
- While scientists agree that THC impairs driving performance, the level of THC in bodily fluids cannot be used to reliably indicate the degree of impairment or crash risk;
- Whereas evidence was gathered over many years to arrive at an established metric for alcohol intoxication – Blood Alcohol Concentration (BAC) – these types of data do not exist for cannabis;
- In contrast to alcohol, THC can remain in the brain and body of chronic, heavy users of cannabis for prolonged periods of time (sometimes several days or weeks), far beyond the period of acute impairment, potentially contributing to a level of chronic impairment;
- Some heavy, regular users of cannabis, including those who use cannabis for medical purposes, may not show any obvious signs of impairment even with significant THC concentrations in their blood. Conversely, infrequent users with the same or lower THC concentrations may demonstrate more significant impairment;
- There is a significant combination effect when cannabis is consumed with alcohol, leading to a greater level of intoxication and motor control problems than when either substance is consumed alone;
- Roadside testing tools to measure THC presence in a driver’s system are in development. Oral fluid screening devices are the most advanced today (and have the added advantage of signalling recent use);
- Other challenges exist, including the need to account for the rapid and sharp decline of THC levels in the blood in the hours following consumption through smoking (with edibles the decline is more gradual).
Most experts agreed that, despite these uncertainties, setting a per se limit for THC blood levels, which establishes a universally applicable level deemed to be consistent with significant psychomotor impairment and increased risk of crash involvement, would be a useful tool to deter cannabis-impaired driving. A per selimit, as is the case for alcohol, would simplify enforcement and adjudication by eliminating the need to prove, on a case-by-case basis, that a driver was impaired.
However, there was little agreement among experts on what that limit should be. More research is needed to help define an acceptable per se limit for THC that would be based on the same robust scientific testing and epidemiological research that supports the per se laws in place for alcohol.
By comparison, per se limits instituted in jurisdictions which have legalized cannabis for medical and non-medical purposes lack standardization in both the impairment threshold and the type of fluid collected and tested. Some jurisdictions use a blood sample while others require urine or oral fluid samples, and THC concentrations vary depending on which bodily fluid is tested. Thus, depending on the fluid used, per se limits in place range anywhere from 1 μg/L to 10 μg/L.
Some jurisdictions have taken alternative approaches to the use of a per se limit to assess and control cannabis-impaired driving. The first approach is the “zero tolerance” policy, which is a variation on the per se limit in which the legal limit is set at zero (or at low detectable levels). This approach is often used in jurisdictions where cannabis continues to be illegal.
The second approach is the “effect-based” approach, which involves proving through various assessment methods that cannabis has impaired the driver’s ability to operate a vehicle. This is the system currently used in Canada. Drivers demonstrating impaired performance during a standardized field sobriety test (SFST) are then obliged to undergo an additional evaluation by a Drug Recognition Expert (DRE) who is properly trained and better able to detect impairment of drivers under the influence of cannabis or other drugs.
We were informed that DRE training for Canadian law enforcement is expensive, time-consuming, requires travel to the United States and is currently only available in English. As a result, few officers have been trained, resulting in insufficient capacity to deal with the current rates of drug-impaired driving. Other challenges include limitations on drawing blood and proving the impaired driving offence at trial.
Some experts called for a “general impairment” test that is not drug-specific. They argued that the real issue is impairment rather than the presence of any compound in the bodily fluid tested. There was also concern that frequent users, in particular medical users, may be impacted disproportionately.
There were repeated calls for funding and additional research in several areas, including:
- To better link THC levels to impairment, which could support the development of a per se limit;
- To develop effective and reliable roadside testing tools to detect THC levels and help law enforcement enforce the rules that are put in place; and
- To hire and train more DREs and officers able to conduct SFSTs.
In addition to the need for better detection techniques, we were also told about the importance of deterrence. Experts stated that the knowledge that impairment could and would be detected, coupled with the certainty of swift and meaningful sanctions, was the most effective way of deterring unwanted driving behaviours.
Additionally, many stakeholders advocated for implementing a public education campaign to inform Canadians about the risks of cannabis use while driving. The link was made to successes in reducing alcohol-related collisions in the late 20th century through robust and ongoing public education campaigns. Many also noted that public education campaigns should be targeted at youth, given their propensity to both use cannabis and be involved in automobile accidents. Recent public opinion research has shown a disturbing trend among youth of a lack of understanding of the effects of cannabis use and impairment. A significant proportion of youth believes that cannabis use leads to more cautious driving and that it is difficult for police to detect and charge drivers for cannabis-impaired driving. In fact, we heard that high school-aged drivers are far more likely to drive following cannabis use than after drinking alcohol.
There were repeated calls to continue to treat impaired driving as a serious criminal offence, especially in cases involving property damage or injury/death.
Many stakeholders recommended that other tools be made available in addition to criminal sanctions, such as graduated https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative penalties (e.g., licence suspensions, vehicle seizure, mandatory education, ticketing), supported by assessment, treatment and rehabilitation programs. These measures have proven effective in changing behaviours with respect to alcohol-impaired driving and also serve to reduce the burden on the justice system.
Considerations
The Task Force agrees with experts in law enforcement that impaired driving is a serious issue that exists currently and requires immediate action to protect public safety.
We acknowledge the clear need for investment in detection and enforcement tools. Most importantly, investment in research to link THC levels to impairment and crash risk is required to support the establishment of a scientifically supported per se limit. In addition, investments to support the development of accurate and reliable roadside testing tools are required.
Despite uncertainty with the current scientific evidence around a per se limit, establishing one would nevertheless be an important tool for deterring cannabis-impaired driving. As the scientific knowledge base continues to grow, a per se limit should be revisited and adjusted as necessary.
Medical cannabis patients expressed concern about how a per se limit could negatively affect them and sought special consideration. We are aware that the United Kingdom has instituted a medical exemption from their per se laws. However, it is important to note that this exemption only applies to the per se offences. A medical patient, regardless of the circumstances, could still be prosecuted for impaired driving.
A particular challenge with a per se limit is that it implies that it is acceptable to consume up to the established limit. Yet there is currently no evidence to suggest there is an amount of THC that can be consumed such that it remains safe to drive. Therefore, a per se limit must be reinforced by strong public education messaging on the dangers of impaired driving. It is clear that the best way to avoid driving impaired is to not consume before or while driving.
The Task Force would like to acknowledge the ongoing work of the Drugs and Driving Committee (the DDC), which is a committee of the Canadian Society of Forensic Science (CSFS), a professional organization of scientists in the various forensic disciplines. The DDC acts as an advisory body to the Department of Justice on issues relating to drug-impaired driving and has been given a mandate to develop reports regarding drugs that are proposed for zero-tolerance and per se legislation, including cannabis/THC. The complexity of this issue is underscored by the fact that the DDC has devoted significant time to exploring per selimits for THC. Its report to Government is still in development.
Given its ongoing work and the lack of consensus on this issue, the Task Force hopes that our considerations help inform the DDC’s important work.
Cannabis-impaired driving should continue to be dealt with through federal criminal law, including more serious penalties for impaired driving causing injury or death. To deter cannabis-impaired driving among youth and new drivers, provincial and territorial governments should consider implementing a policy of zero tolerance for the presence of THC in the system of new or young drivers.
The use of SFSTs and DRE evaluations will continue to be the primary tool used by law enforcement to enforce cannabis-impaired driving laws until such time that a scientifically supported per se limit is established and a reliable roadside testing device is available for use. However, as noted by stakeholders, investment in DRE training and staffing is currently insufficient. Significant and additional resources are required to better equip law enforcement to detect impaired drivers and enforce the rules.
The Task Force believes that impaired driving needs immediate action through stable, ongoing investments in law enforcement to train, certify and hire more DREs and to ensure more officers are able to conduct SFSTs to assess impairment at the roadside. This could include developing a bilingual training and certification program in Canada. Once a suitable roadside testing device is developed, investments will also be necessary to deploy it nationally.
To complement the implementation of a system of penalties and enforcement, a robust and ongoing national public education campaign requires proper funding and implementation as soon as possible, prior to legalization. Its focus should be on the dangers of impairment caused by cannabis use and how to use responsibly. The public education campaign must be evidence-informed and should include a focus on the dangers of impairment more broadly.
As with current messaging for drinking and driving, the campaign should reinforce the message that cannabis use and driving should not be combined. The public education campaign should include messaging on the increased risks of using cannabis in combination with alcohol. Messaging also needs to reinforce that law enforcement has the capability to detect cannabis use through the SFST and DRE evaluations and that sanctions that carry serious consequences will be imposed.
Furthermore, the public education campaign needs a special focus on youth to dispel the myth that cannabis use leads to better driving.
Finally, co-ordination among the federal, provincial and territorial governments will be key to a successful public education campaign.
It will be essential to establish a baseline in order to accurately monitor and assess the impact of legalization on impaired driving. Ongoing surveillance and information sharing among all jurisdictions will build an evidence base to support adjustments to the system as trends and new evidence emerge. We recommend that governments make investments in this regard.
Advice to Ministers
The Task Force recommends that the federal government:
- Invest immediately and work with the provinces and territories to develop a national, comprehensive public education strategy to send a clear message to Canadians that cannabis causes impairment and the best way to avoid driving impaired is to not consume. The strategy should also inform Canadians of:
- the dangers of cannabis-impaired driving, with special emphasis on youth; and
- the applicable laws and the ability of law enforcement to detect cannabis use
- Invest in research to better link THC levels with impairment and crash risk to support the development of a per se limit
- Determine whether to establish a per se limit as part of a comprehensive approach to cannabis-impaired driving, acting on findings of the DDC
- Re-examine per se limits should a reliable correlation between THC levels and impairment be established
- Support the development of an appropriate roadside drug screening device for detecting THC levels and invest in these tools
- Invest in law enforcement capacity, including DRE and SFST training and staffing
- Invest in baseline data collection and ongoing surveillance and evaluation in collaboration with provinces and territories
The Task Force further recommends that all governments in Canada consider the use of graduated sanctions ranging from https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative sanctions to criminal prosecution depending on the severity of the infraction. While it may take time for the necessary research and technology to develop, the Task Force encourages all governments to implement elements of a comprehensive approach as soon as feasible, including the possible use of https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative sanctions or graduated licensing with zero tolerance for new and young drivers.
Chapter 5: Medical Access
Introduction
The regulatory framework proposed by the Task Force for non-medical cannabis is influenced by prior medical regimes – in particular, through the establishment of safeguards for product quality and security and of safety provisions to prevent diversion.
The courts have recognized the rights of patients to access cannabis for medical purposes. The Canadian context dates back to the late 1990s and the first constitutional challenges to the Government’s general prohibitions on access to cannabis. Patients argued that the prohibitions in the Controlled Drugs and Substances Act forced them to choose between their liberty and access to a necessary medicine, which was often supplied by compassion clubs and medical dispensaries that emerged to support the therapeutic use of cannabis.
In order to preserve the general prohibitions, the Government allowed access for medical purposes. Starting in 1999, this was achieved by issuing exemptions to allow individuals access on an exceptional basis. This exemption-based scheme was challenged and found to be deficient by the courts and was replaced in 2001 by a regulatory framework.
However, patients subsequently contended in a series of successful court challenges that the Marihuana Medical Access Regulations (MMAR) placed a number of unreasonable limits on their access to cannabis. The regulations were amended a number of times to address these constitutional deficiencies and ultimately were replaced, in 2014, by a new framework known as the Marihuana for Medical Purposes Regulations (MMPR). Unlike the MMAR, where patients could cultivate to supply their personal medical needs or designate someone to do so for them, the MMPR was based solely on commercial production, whereby individuals requiring access could purchase quality-controlled product from a producer licensed by Health Canada.
In a constitutional challenge to the MMPR, Allard v. Canada, the plaintiffs argued that the elimination of personal and designated person cultivation as had existed under the MMAR limited the availability and affordability of their medication. In its 2016 decision, the Federal Court of Canada declared the MMPR unconstitutional on the basis that it did not provide patients with reasonable access to cannabis – that is, a reasonable choice of strains available at adequate prices and in the quantity required to meet medical needs.
In response, and during our consultations, the Government introduced new regulations, the Access to Cannabis for Medical Purposes Regulations (ACMPR), in August 2016. In addition to maintaining the system of access provided by licensed producers, the ACMPR provide patients with options to produce their own supply of cannabis for medical purposes in accordance with the daily amount outlined by their physician, to designate someone else to do so, or to purchase cannabis from a producer licensed by Health Canada.
While the Task Force was not involved in the development of the ACMPR, in formulating our advice on the future of medical access we have considered how this latest iteration of the Government’s medical access regime works and how it is perceived by those most impacted by it.
One system or two?
While stakeholders appreciate that the formal clinical evidence base is incomplete, there is agreement that many individuals suffering from a variety of serious medical conditions derive therapeutic benefits from both THC and CBD. This makes these patients’ use of cannabis different from that of non-medical users, even though the product (dried cannabis, cannabis oil, etc.) being used is the same.
While there was general agreement on the legitimacy of medical use, there were two very different perspectives as to the need for a separate system for medical access to cannabis. We recognize that these perspectives and views were shaped by the system that exists today – a system that is an exemption or carve-out to the general prohibitions that are otherwise in place.
On the one hand, there is a view that a separate system is necessary to preserve medical access. This is the dominant view of patients, who related to us the decades of effort, most often through court challenges, to gain access to cannabis for medical purposes. While acknowledging that cannabis for non-medical purposes will be legal and more broadly available for those who choose to use it, patients stressed that they use cannabis out of necessity, not choice.
Patients expressed concerns that their needs would not be accommodated in the new system and that the access rights they have today could be lost. The following issues emerged as key areas of concern for them: the loss of recognition that their use of cannabis is for medical purposes and occurs under the supervision of a physician; shortages of supply; barriers for young people; and the stigma associated with having to purchase cannabis for medical purposes from a non-medical retail outlet.
On the other hand, we heard that there is no need for a separate system, as the end of prohibition will mean that those who need to access cannabis for medical purposes will be able to do so legally. This is the prevailing view of members of the medical community, who have long-standing concerns about being responsible for authorizing the use of a substance that is not an approved medicine and who see no need to play the role of “gatekeeper” moving forward. We also heard about the potential challenges posed by the operation of dual systems, both from an https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative and an enforcement perspective. Law enforcement and municipal representatives warned against perpetuating the abuse of licences to create large-scale grow operations.
Access
During our consultations, we heard many compelling personal stories of how cannabis is making a difference to Canadians living with serious health challenges such as cancer, HIV/AIDS, multiple sclerosis, arthritis and fibromyalgia. We also heard about the role that cannabis can play in pain management and palliative care, and the relief that cannabis, particularly strains with high levels of CBD and low levels of THC, offers to children with severe forms of epilepsy.
We also learned that many individuals have come to use cannabis for medical purposes after exhausting other conventional treatments and medications. Several patients told us that their use of cannabis has enabled them to limit or eliminate their use of powerful narcotic drugs such as opioids.
These patients and their advocacy organizations worry that the access they have today will disappear under a system that does not acknowledge medical use as separate and distinct from non-medical use. In their view, removing the prohibitions on cannabis and moving to a single, non-medical system does not acknowledge the legitimacy of medical use nor the reasonable access rights that have been recognized by the courts.
Affordability
Many patients cited the high costs they incur today in purchasing cannabis from licensed producers. We heard that it is not uncommon for patients to spend hundreds or thousands of dollars each month in order to acquire a sufficient supply of cannabis. This cost burden is compounded by the fact that, unlike prescription drugs, medical cannabis is neither exempt from the Goods and Services Tax (GST) nor eligible for reimbursement under public or private insurance plans (with very limited exceptions).
Patients worry that these costs would continue, or rise, due to new taxes or other price controls. We heard suggestions that the Government should, within a continued medical access system, support patients by “zero rating” medical cannabis under the Excise Tax Act, thereby eliminating the GST on its sale, and facilitate insurance coverage by recognizing cannabis as a drug or “drug equivalent.”
Products
We heard a great deal of concern about availability, or the ability to access cannabis in the amount required, when required. Patients were concerned that they would lose access to their preferred strains of cannabis, particularly those likely not to be of interest to the recreational user (e.g., strains with low levels of THC). We were told about the product shortages that occur today, especially for cannabis oil, and concern that these shortages could be more prevalent in the future unless measures were taken to prioritize the needs of medical users.
Patients were also concerned about losing access to high-potency strains or product types that they currently use, either because of THC potency limits or cost barriers associated with a taxation structure based on THC potency.
For many patients who raised these affordability and availability concerns, the preservation of access through personal cultivation for medical purposes is crucial. The maintenance of personal cultivation is also key to those who have concerns with the quality of product from licensed producers and those who, for example, wish to grow pesticide-free plants.
While personal cultivation meets the needs of some medical users, there were many others who told us they prefer a commercially produced product. We heard from medical users who are satisfied with the quality and choice offered by licensed producers, the support and assistance they receive and the convenience and relative anonymity of mail-order delivery. Several licensed producers told us about the investments they have made in their production infrastructure, plant genetics research and strain development, as well as the efforts they have made to meet the needs of a diverse patient base, whether through customer support or compassionate pricing programs.
Many patients expressed concern with the limitations of the existing mail-order model, including the interruptions in supply resulting from the time required to ship and deliver cannabis once it is ordered. We heard that patients would benefit from in-person contact with educated and trained staff to discuss issues such as choice of strains and method of consumption. Patients were clear that there should be a dedicated medical access retail option, protecting them from, among other things, the potential stigma of having to disclose personal medical information in a non-medical retail environment. Some not-for-profit, holistic, individual-centred services exist and are seen to be of benefit to patients.
We are aware that national pharmacy associations and several major pharmacy chains have an interest in dispensing cannabis for medical use. They note that Canadians think first of pharmacies when they think of where to purchase medicine and that pharmacies have systems and infrastructure in place to safely handle and store narcotic drugs in accordance with federal regulations. These organizations also highlight the broad reach of pharmacies, including in rural Canada. We heard from them that pharmacists, as health professionals and experts in medication management, are well-placed to support patients. However, we are also aware that many pharmacists feel that they do not have the clinical training or information to properly advise and counsel patients on issues such as drug interactions, contraindications or potential dependence. Several of the provincial and territorial regulatory and licensing authorities for pharmacists indicated that pharmacy distribution should not be considered until there is additional clinical research demonstrating the therapeutic value of cannabis and until cannabis has been approved for sale by Health Canada as a drug.
Public safety
We heard from municipalities and law enforcement, in particular, about the abuse of cultivation provisions under the MMAR and concern that the ACMPR will be exploited in the same way.
These stakeholders relayed numerous examples of instances where licences issued under the MMAR, notably those to designated producers, were effectively used as a cover for illegal production and diversion to the illicit market. We heard about the size and scale of some of these designated producer operations and instances where law enforcement encountered thousands of plants in residential properties. Representatives from municipalities told us about the challenges these grow operations pose to neighbours, landlords and communities because of fires, break-ins and rental properties rendered uninhabitable due to mould or other contaminants.
Evidence and research
The lack of information to guide clinical decision-making on the use of cannabis was the dominant theme of our discussions with the medical community.
Physicians and their regulators reminded us that the medical access system in place today not only serves as an exemption or carve-out to the prohibitions in the CDSA but also to the Food and Drug Regulations under the Food and Drugs Act (FDA).
This has placed physicians in the difficult position of being responsible to support patient use without a full understanding of benefits and risks to their patients, as they would have for any other prescription drug. While they recognize that some patients may obtain relief from their symptoms through the use of cannabis, they told us that it is difficult to meet their obligations to provide patient care and to protect patient safety when they do not have the evidence, training or guidance to do so. As a result, many physicians are unwilling to support the use of cannabis as a treatment, leaving some patients unable to secure the medical authorization needed to purchase or produce cannabis.
For this reason, both the Canadian Medical Association (the national association representing physicians) and the Federation of Medical Regulatory Authorities of Canada (the national association representing medical regulators) have expressed clear positions that it is not appropriate for physicians to continue to authorize access to cannabis. These associations believe that the removal of the prohibitions under the CDSA will eliminate the need for the medical access system as it exists today, including the requirements for physician authorization.
They suggest that reasonable access for medical purposes can be met through a single, non-medical system and that patient needs for information and advice could be fulfilled at point of sale by those involved in retail distribution. The medical establishment acknowledges that provisions would need to be made to accommodate minors requiring cannabis for medical purposes, as minors would otherwise be excluded from access.
The medical community also noted that there are cannabinoid-based medicines that meet the regulatory threshold of approval for sale as a prescription drug, meaning that they can be marketed for sale with claims as to safety, efficacy, quality and use for certain conditions. Physicians have standardized information about these drugs and are able to properly advise patients on issues such as interactions with other medication and adverse effects. They point to the presence of these prescription medications as evidence that the existing drug approval process can and should be used moving forward, leading to more cannabis- and cannabinoid-based drugs being prescribed by physicians and dispensed by pharmacists.
It was further suggested that the removal of the prohibitions on cannabis may help to create an incentive for the research that is needed to meet the FDA threshold of evidence, whether by licensed producers or others. It was suggested to us that the Government could do more to incentivize and incubate this research, possibly through funding agencies such as the Canadian Institutes of Health Research (the federal agency mandated to invest in health research), and could actively promote the existing FDA approval process for cannabis- and cannabinoid-based products. Proponents point out that this approach, which would lead to products with market authorization and associated Drug Identification Numbers (DINs), would address some of the affordability issues cited by patients, since drugs with a DIN are eligible for reimbursement under public and private insurance plans.
Some stakeholders, including a number of patients, suggested that the Government create a standalone pathway for the approval of cannabis medicines, leading to DINs or DIN-equivalents, in certain circumstances. Other stakeholders asserted that the approval process used for natural health products would be appropriate to use for cannabis, given that it is a herbal medicine. However, there was acknowledgement that the natural health products regime might not adequately accommodate the ways in which cannabis is used to treat certain serious conditions and that natural health products do not typically qualify for insurance coverage.
Patients underscored that industry would be unlikely to invest in clinical drug development research without the presence of, and a pathway to, a dedicated medical market. There was particular concern that there would be little research into CBD-rich strains of cannabis that have potential medical applications, leaving patients to accommodate their medical needs with products aimed at non-medical users.
Considerations
In considering our recommendations on medical access and cognizant of our guiding principles, we aimed to promote the following:
- Continuing to provide patients with reasonable access to cannabis for medical purposes, such that they can acquire and use cannabis to meet their needs while not facing undue constraints of cost or choice;
- Supporting the medical community with ongoing research and evidence on the therapeutic benefits and risks of the use of cannabis for medical purposes; and
- Contributing to the integrity of the overall cannabis framework that the Government will establish and minimizing the potential for abuse and diversion.
While the current medical access system is not without its challenges, we understand that the ACMPR provide patients with the flexibility to access cannabis in the way that best meets their medical needs and accommodates their personal circumstances, whether that be from licensed producers or personal cultivation. However, we did hear concerns that the legitimacy of the system has been compromised by the continued presence of persons designated to cultivate for medical users, many of whom have exploited their status for illicit gain at the expense of the communities in which they are located.
As such, and in light of the extent of the change that is to come, we believe that the Government should maintain the ACMPR, with some modifications, at the outset of the new system of regulated legal access. This represents a sensible means of preserving patient access at a time of unprecedented change, but it must be complemented by increased research and evidence about cannabis for medical purposes. We further believe that the Government should re-evaluate the ongoing relevance and need for the medical access system in five years.
We recognize that, in the interim, patients may be concerned as to whether licensed producers will continue to be able to supply their needs if they are permitted to supply the non-medical market. Patients may also be worried about the impact of a new tax scheme applicable to all cannabis products. It will be imperative for the Government to monitor patient access closely as the new system for legal access to cannabis is implemented. The Government will need to work closely with licensed producers and patients to identify and address emerging issues and take decisive action if required, whether requiring licensed producers to prioritize supply for medical users or establishing price controls for medical users. The Government should take the necessary steps to have the authority to regulate these issues moving forward, while being mindful that executing these authorities may create the potential for market distortion and exploitation as individuals seek to benefit from perceived advantages in the medical regime.
In the interests of patients, however, the Government should be prepared to expedite other broad changes to the regime should monitoring reveal that reasonable access is being compromised. This could include pharmacy distribution, although we recognize that making such a change would also require regulatory changes at the provincial and territorial level, given the role that provincial and territorial regulatory and licensing authorities play in regulating the scope of practice of pharmacists. We would encourage the Government to engage in discussions with provinces and territories, the regulatory and licensing authorities, pharmacy associations and other implicated stakeholders to explore the feasibility of this approach.
We understand that there are valid concerns about the potential for abuse of the personal cultivation provisions of the ACMPR, particularly by those without medical needs or who use medical needs as a shield for illicit activity. However, on balance, we accept that personal cultivation can be done safely and responsibly, without risk to the patient or to others, and we acknowledge the role that it plays for medical users who otherwise would be prevented from acquiring cannabis because of its cost.
However, the Task Force believes that the Government should respond to the concerns expressed by municipalities, law enforcement officials and community members by immediately reviewing the current risks associated with designated production and the ongoing need for such production. There should be a sufficient range of options available to patients in the future to easily access cannabis for their medical need. The majority of Task Force members believe that the problems with the activities of some designated producers are serious and that the Government should determine an appropriate timeframe for phasing out this provision as the new system for non-medical uses of cannabis is established.
We appreciate the hesitancy of the medical community to participate in authorizing cannabis for medical purposes under the ACMPR and understand that this creates a barrier to access for some patients. It is clear to us that both physician and patient interests will be served by advancing science and research on the therapeutic uses of cannabis and associated issues relating to dosage, potency, consumption methods, interactions with other medicines and adverse effects. As the CMA noted in its submission to the Task Force, “It is important that there be support for research of cannabis in order to develop products that can be held to pharmaceutical standards.”
Although we heard some support for the Government to incentivize this research by creating a new, standalone pathway for the approval of cannabis medicines, we believe that there is a place for cannabis- and cannabinoid-based medicines under the existing FDA drug approval process for prescription medications. With approvals, these medicines could be marketed with claims as to their safety, efficacy and use, and be exempt from GST, like other prescription drugs. With market authorization and DINs, these medicines would become eligible for inclusion on public and private drug formularies and insurance plans, thereby addressing the affordability barriers about which we heard.
Some companies may wish to market cannabis products as “wellness products” rather than as medicines. We understand that the federal government is currently conducting a review of its approach to the regulation of natural health products. The question of CBD or other non-psychoactive cannabinoids as potential wellness products is likely to be explored in this review process and will be informed by emerging research in this area.
The Government must work with industry, the medical community and the patient community to promote and encourage clinical research and drug approval submissions for cannabis- and cannabinoid-based products. Although industry has a significant role to play here, there may be merit to the Government investing in targeted research in this area, potentially through agencies such as the Canadian Institutes of Health Research.
We recognize that this work will take time and, in the interim, it is incumbent on the Government to take steps to ensure that both physicians and patients have access to clear, non-biased, non-promotional, evidence-based information to assist in decision-making. We see a vital need for governments to work with the medical community on issues such as medical school curricula, continuing medical education and training. Furthermore, governments must, as part of their broader education initiatives, ensure that material is developed and made available to support patients in their use of cannabis for medical purposes.
Advice to Ministers
The Task Force recommends that the federal government:
- Maintain a separate medical access framework to support patients
- Monitor and evaluate patients’ reasonable access to cannabis for medical purposes through the implementation of the new system, with action as required to ensure that the market provides reasonable affordability and availability and that regulations provide authority for measures that may be needed to address access issues
- Review the role of designated persons under the ACMPR with the objective of eliminating this category of producer
- Apply the same tax system for medical and non-medical cannabis products
- Promote and support pre-clinical and clinical research on the use of cannabis and cannabinoids for medical purposes, with the aim of facilitating submissions of cannabis-based products for market authorization as drugs
- Support the development and dissemination of information and tools for the medical community and patients on the appropriate use of cannabis for medical purposes
- Evaluate the medical access framework in five years
Chapter 6: Implementation
“This is about the hardest, most complicated thing in public life that I’ve ever had to work on.”
– Colorado Governor John Hickenlooper, from interview with 60 Minutes, broadcast on October 30, 2016
As this report makes clear, the regulation of cannabis is a complex public policy issue and, as with other complex policy issues, the depth and scale of the complexity increases as we turn to the practicalities of implementation.
As governments determine how to roll out the new system, there are many aspects to consider, including:
- The kinds of capacity and infrastructure governments will need to develop or expand, and in what areas;
- The kinds of oversight that are necessary during implementation, including monitoring, evaluation and review;
- How different levels of government will work together, including with municipalities and Indigenous governments and representative organizations; and
- What communication with the public is required, and when.
It will be a challenge for governments to manage the period between the coming into force of federal legislation, at which point cannabis will be legal, and the creation of regulations for the regime (in addition to the passing of provincial and territorial legislation and regulations). Some provinces and territories have urged that this period be as short as possible, to limit the growth of unregulated commercial activity. While there are likely to be calls for special measures during this period, such as decriminalization of cannabis, governments should focus on the long-term success of the system. It will be necessary for governments to co-ordinate efforts in order to implement the regime as quickly as possible. Public education and clear and regular communications will be critical during this period.
Capacity
Canada’s governments, and many other organizations, will need to work quickly to prepare for the implementation of the new system, increasing or developing capacity in many areas relating to production, distribution and retail, quality control and enforcement, and research and surveillance. This increase in capacity will require new resources (human and financial), enhancements to existing institutions and the creation of new ones. Having all elements in place will be necessary for the proper functioning of the regime. Some, such as infrastructure for distribution and retail, will be the domain of the provinces and territories. The Task Force recommended earlier in this Report that the federal government should increase capacity in areas such as prevention and treatment programs for individuals suffering from dependence. Federal investment will also be needed in research and surveillance, laboratory testing, licensing and regulatory inspection and training to increase capacity ahead of regulation; these elements are outlined below.
National funding for research and surveillance: Research is critical to the regulated cannabis regime in two critical ways: surveillance, to monitor the progress and efficacy of the regulatory measures; and research, to provide a better understanding of the benefits and harms of cannabis. There is overlap between these areas – for instance, both surveillance and research can be used by governments to adjust and improve the regulatory regime. The legalization of cannabis provides an opportunity to develop the knowledge base in both areas, but federal leadership and funding will be essential. (More information on the collection and use of surveillance data is in the “Oversight” section below.)
As a result of long-standing prohibition, the study of cannabis is decades behind that of legal therapeutic substances such as opioids, but plans are underway to improve this situation. In the fall of 2016, members of the Task Force attended a number of meetings of researchers who are identifying knowledge gaps on non-medical cannabis and identifying priorities for future research. These include research on scientific and medical aspects (e.g., the effects of cannabis on the brain and behaviour and better understanding the endocannabinoid system), public health (e.g., psycho-social impacts of cannabis) and drug-impaired driving (e.g., questions around per se limits, impairment detection and measurement).
Our Report recommends dedicating a portion of government revenues to research, but funding in this area should start early. Governments should also encourage research-granting councils to establish cannabis research as a priority and encourage the academic and private sectors to contribute to research funding.
The Task Force is also aware that the World Health Organization has not conducted a systematic review of cannabis since 1935. Given the global dialogue on cannabis reform, we think it appropriate that Canada, as part of its international engagement, call on the WHO to conduct a new systematic review.
Establishing and promoting laboratory standards: Laboratory testing is a cornerstone of some of the health and safety measures proposed in Chapter 2. Specifically, the mandatory product testing recommended by the Task Force is intended to minimize the risk of contaminated products entering the market and to verify the information on labelling, in order to help consumers make informed decisions. Canada is in the fortunate position of having laboratory standards for cannabis as part of the existing medical cannabis program; as noted in Chapter 3, the capacity of this system will need to be adapted to a new regulatory environment and enhanced so that licensed producers can meet new product safety, quality and labelling requirements. The federal government will play a key role in facilitating this enhancement and ensuring it is capable of meeting the needs of the new regime.
Licensing and inspection: To be effective, a regulatory regime’s requirements must be enforced. Governments will need to ensure that they have the resources and tools in place to do so. This will include building capacity for licensing and inspection at all levels of government: federal (e.g., for production and laboratories), provincial and territorial (e.g., for distribution and retail), and municipal (e.g., for home-cultivation permits).
At the federal level, the existing inspection system for medical cannabis could serve as a solid foundation to meet the needs of the new framework but would need to be appropriately resourced and expanded. In addition, it will be important that the Government ensure adequately resourced and timely federal licensing capacity, including processing of licence applications and facilitating access to seeds for production.
Training: Those who enforce the new regime – including police, who enforce the criminal law, and government inspectors, who verify that companies and individuals are complying with regulations – will need proper training to be able to do their jobs. While all levels of government will be involved in training officials within their respective jurisdictions, we can expect that most will look to the federal government for leadership in setting standards and developing content for such training.
Advice to Ministers
The Task Force recommends that the federal government:
- Take a leadership role to ensure that capacity is developed among all levels of government prior to the start of the regulatory regime
- Build capacity in key areas, including laboratory testing, licensing and inspection, and training
- Build upon existing and new organizations to develop and co-ordinate national research and surveillance activities
- Provide funding for research, surveillance and monitoring activities
Oversight
To be satisfied that the system is minimizing harms and maximizing benefits as intended, it will need close monitoring, at least initially. This will require data gathering, measurement, analysis and reporting of results. The results of this process will allow governments to make adjustments, based on timely evidence.
Surveillance and Monitoring: Surveillance and monitoring of the regime will be done in different ways. Government regulators will monitor the market – producers, retailers and other participants – to verify that products and processes meet requirements. Surveillance also refers to monitoring population-level indicators, such as patterns of use, age of initiation and use of cannabis with tobacco, alcohol and other drugs. To measure the impact of changes, governments will need to establish “baseline” indicators prior to legalization. We heard from several stakeholders, as well as U.S. states such as Colorado, that gathering this baseline data should be an immediate priority and begin prior to implementation.
Fortunately, work is underway in Canada to prepare for this. The Canadian Institutes of Health Research held a workshop in October 2016 to examine baseline data needs and, as a first step, the federal government is planning a new national cannabis survey to obtain more comprehensive data on cannabis use.
The federal government should work with provincial, territorial and municipal governments on the sharing of data from their respective jurisdictions. Sources of this data may include sectors such as health care (e.g., visits to emergency departments and hospitalizations), law enforcement (e.g., police-reported incidents and charges), industry (e.g., cultivation and manufacturing data) and transportation (e.g., traffic accident data).
An example of the importance of co-ordination and data sharing is in relation to poison control centres – provincial and territorial services that help the general public and health-care practitioners seek guidance and medical advice for treatment of poisonings, chemical intoxications and adverse drug reactions. They are an important data source given the risk of accidental ingestion of cannabis products. However, calls to the centres are not systematically aggregated or analyzed nationally, and there is a recognized need to integrate their information to provide a national picture. Efforts are underway to provide national-level data associated with cannabis exposures (and other substances) and to develop a baseline before regulation.
Evaluation: As noted above, data will be needed to track the evolution of the new system. Analysis that compares data gathered from surveillance activities under the new system against baseline data will help regulators determine whether we are on track to achieve the goals of reducing use by youth and reducing the profits of the illicit industry.
Timely data collection, evaluation and reporting of results will be key to the successful development of the system.
Advice to Ministers
The Task Force recommends that the federal government:
- Establish a surveillance and monitoring system, including baseline data, for the new system
- Ensure timely evaluation and reporting of results
- Mandate a program evaluation every five years to determine whether the system is meeting its objectives
- Report on the progress of the system to Canadians
Co-ordination
For this system to be successful, federal, provincial, territorial, municipal and Indigenous governments will need to work together on information sharing, including the data required for oversight, and on the co-ordination of efforts to set up all of the components of the new regime, including production, distribution and retail. Provincial and territorial officials who met with the Task Force saw close co-ordination on the rollout as essential.
Canada should prioritize engagement of Indigenous governments and representative organizations regarding their interests, perspectives and roles as the new system is designed and implemented. The Task Force also heard from Indigenous leaders and organizations of their interest in participating in the forthcoming cannabis market and of economic opportunities which may contribute to creation of new jobs in their communities. A particular interest of Indigenous representatives is the opportunity for Indigenous governments or individuals to acquire cannabis production and distribution licenses.
There exists in Canada a strong and well-informed base of organizations, advocates, charities, foundations and other stakeholders who have advanced cannabis-related research and policy work. These groups can be relied upon as important sources of knowledge and advice as governments move forward to enact the new system. Non-governmental organizations will play an important role in the implementation of the new system.
Advice to Ministers
The Task Force recommends that the federal government:
- Take a leadership role in the co-ordination of governments and other stakeholders to ensure the successful implementation of the new system
- Engage with Indigenous governments and representative organizations to explore opportunities for their participation in the cannabis market
Communication
Governments should communicate early, clearly, consistently and often to Canadians about the new system. Youth and parents will need the facts about cannabis and its effects. Actors in the new system – including employers, educators, law enforcement, industry and others – will require information tailored to their specific roles. As such, communication can serve multiple purposes:
- Public education campaigns (see Chapter 2), including information for schools to help them adjust curricula;
- Information to help consumers make informed choices;
- Information for the public on how the regulation of cannabis “works” – what is allowed, what is not, and why, including during the interim period before the system is operational;
- Guidance for health-care practitioners on the medical use of cannabis, updated regularly to account for new research;
- Guidance for municipalities, law enforcement, employers and others on their roles and responsibilities under the new system; and
- Information for industry on licensing and other rules for their participation in the regulated system.
Funding will be required early to ensure a public education campaign is implemented ahead of legalization. Messaging on harms and benefits will need to be co-ordinated among different governments and shared with industry and advocacy groups. The results of oversight will need to be communicated with Parliament and the public. Canada should expect strong interest from the international community and be prepared to share information on its approaches, data and lessons learned.
Advice to Ministers
The Task Force recommends that the federal government:
- Provide Canadians with the information they need to understand the regulated system
- Provide Canadians with the facts about cannabis and its effects
- Provide specific information and guidance to the different groups involved in the regulated cannabis market
- Engage with Indigenous communities and Elders to develop targeted and culturally appropriate communications
- Ensure that Canada shares its lessons and experience with the international community
Annex 1: Biographies of Task Force on Cannabis Legalization and Regulation Members

The Honourable A. Anne McLellan (Chair)
The Honourable A. Anne McLellan, P.C., O.C., A.O.E. joined Bennett Jones LLP in its Edmonton Office in July 2006. She serves on the Board of Directors of Agrium and Cameco. Among her many community commitments, she serves on the Board of the Edmonton Community Foundation, the Edmonton Oilers Foundation and the Institute for Research on Public Policy. In May 2015, Ms. McLellan became Dalhousie University’s seventh Chancellor.
Ms. McLellan served four terms as the Liberal MP for Edmonton Centre, during which she was Deputy Prime Minister of Canada and Minister of Public Safety and Emergency Preparedness, Minister of Health, Minister of Justice and Attorney General of Canada, and Minister of Natural Resources.
From 1980 – 1992, she was a professor in the University of Alberta’s Faculty of Law and served as both Associate Dean (1985 – 1987) and Acting Dean (1991 – 1992) of the Faculty. Ms. McLellan holds a Bachelor of Arts and a Law degree from Dalhousie University and a Master of Laws degree from King’s College, University of London.
Dr. Mark A. Ware (Vice Chair)
Dr. Ware is an Associate Professor in Family Medicine and Anesthesia at McGill University. He is a family physician and practises pain medicine in Montreal, Quebec. He has a Bachelor’s degree in biochemistry from Queen’s University (BA 1986) and graduated in Medicine from the University of the West Indies (MBBS 1992). He obtained a Master’s degree in Epidemiology from the London School of Hygiene and Tropical Medicine (MSc 1999).
Dr. Ware worked at the MRC Sickle Cell Unit in Kingston, Jamaica from 1996-1998 where he developed his interests in pain management and cannabis therapeutics. Since 2009, Dr. Ware has been the Director of Clinical Research of the Alan Edwards Pain Management Unit at the McGill University Health Centre. He serves as the co-Director of the Quebec Pain Research Network and since 2007 has been the Executive Director of the Canadian Consortium for the Investigation of Cannabinoids (CCIC). He is currently Chairman of the International Association for Cannabinoid Medicine (IACM) and vice-chair of the Scientific Program Committee of the Canadian Pain Society. He has served as an adviser to the Canadian government since 2001 on medical cannabis policy and supporting documents.
He has published over 70 papers on pain and cannabis, six book chapters and given over 150 scientific talks. He was awarded the 2010 Award for Clinical Research Achievement by the IACM.
Dr. Susan Boyd (Member)
Dr. Boyd is a Distinguished Professor in the Faculty of Human and Social Development at the University of Victoria. She has conducted research in the areas of drug policy and law for the last 25 years. She holds a PhD from the School of Criminology, Simon Fraser University and an MA in Clinical Psychology from Antioch University.
Dr. Boyd is the author of seven scholarly books and numerous articles and book chapters in the areas of drug policy and law; cannabis growing and regulation; media representations; heroin-assisted treatment; women, pregnancy, and mothering; the history of drug prohibition; and harm reduction. She is a member of the steering committee for the Canadian Drug Policy Coalition.
Mr. George Chow (Member)
Mr. Chow was a Vancouver City Councillor from 2005 to 2011. Prior to that, he had a 30-year career in engineering. He first got into civic politics in 2002 on the issue of the supervised injection facility in Vancouver’s Downtown Eastside (DTES).
A long-time Vancouver resident, he grew up in DTES and attended Britannia and Gladstone Secondary Schools. He graduated from UBC in mechanical engineering in 1975.
Mr. Chow is a member of the Association of Professional Engineers and Geoscientists of B.C., a Fellow of Engineers Canada and has served on many community organizations as a volunteer, including the Urban Spirit Foundation, Vancouver Public Library Board, Chinese Cultural Centre of Greater Vancouver, Boys and Girls Clubs of South Coast B.C., Chinese Benevolent Association of Vancouver, Vancouver Chinatown Merchants Association and S.U.C.C.E.S.S.
Superintendent Marlene Jesso (Member)
Superintendent Jesso was appointed Officer in Charge with the Combined Forces Special Enforcement Unit Newfoundland and Labrador in 2014. She has 33 years of policing experience, including 10 years in a leadership role enforcing the provisions of the Controlled Drugs and Substances Act (CDSA). Her long-standing approach to CDSA enforcement includes providing both legal and public stakeholders with valuable insight on emerging trends that drugs and drug use present in communities policed by the Royal Newfoundland Constabulary and the RCMP.
Superintendent Jesso has been involved on a national level as a participant in the “Emerging Issues in Drug Enforcement” Workshop with delegates representing law enforcement, justice, academia, and health and social service sectors. She has overseen many highly successful investigations dealing with illegal drugs and organized crime and attributes the success to multi-agency collaboration. Superintendent Jesso was awarded the 30 Year Exemplary Service Award in 2013 and the Queen’s Diamond Jubilee Medal in 2012.
Dr. Perry Kendall (Member)
Dr. Kendall was born in the United Kingdom and received his MBBS in 1968 from the University College Hospital Medical School, London, U.K. In 1983, he received his Master of Public Health from the University of British Columbia and in 1984 became a Fellow of the Royal College of Physicians and Surgeons of Canada.
Dr. Kendall has held a number of Medical Health Officer positions in both B.C. and Ontario including that of Chief Medical Health Officer for the City of Toronto and served as the President and CEO of the Addiction Research Foundation of Ontario from 1995-1998.
In 1999, Dr. Kendall assumed the position of Provincial Health Officer for the Province of British Columbia.
Dr. Kendall has received a number of prestigious awards for his work in public health and harm reductions, including the Order of B.C. (June 2005) and the Queen’s Diamond Jubilee Award (Feb 2013). In 2015, Dr. Kendall was awarded the Legacy Award by the Premier of British Columbia.
Dr. Kendall sits on a number of provincial and national committees, including the Pan-Canadian Public Health Network Council, Council of Chief Medical Officers of Health, B.C. Communicable Disease Policy Committee (Chair), B.C.’s Public Safety Issues Committee on Marijuana Legalization and the Standing Committee on Health Services and Population Health. He is also the Chair of the B.C. Overdose Order Working Group regarding Opioid Overdose deaths.
Mr. Raf Souccar (Member)
Mr. Souccar served as a police officer with the RCMP for 34 years. He retired in 2011 as the Deputy Commissioner responsible for Federal and International Policing. The majority of his career was spent in the area of Drugs and Organized Crime. During that time, he acquired considerable experience not only in the area of drug enforcement but also in the area of Drug Awareness and education for youth and at-risk individuals. Mr. Souccar also led the development of the drug-impaired driving legislation and the creation of the Drug Recognition Expert training for police officers.
Mr. Souccar served as Vice President of the Canadian Association of Chiefs of Police from 2005 to 2010 and co-chaired its Drug Abuse Committee from 2002 to 2005. He was also a member of the International Association of Chiefs of Police Narcotics and Dangerous Drugs Committee from 2003 to 2010.
Mr. Souccar holds a Bachelor of Administration and a Bachelor of Laws (LL.B.) from the University of Ottawa and is a graduate of the University of Toronto Institute of Corporate Directors.
Mr. Souccar is a recipient of several awards, including the Queen’s Golden Jubilee Medal in 2002, the Officer of the Order of Merit of the Police Forces from the Governor General of Canada in 2007, the Queen’s Diamond Jubilee Medal in 2012 and the RCMP Long Service medal.
Dr. Barbara von Tigerstrom (Member)
Barbara von Tigerstrom is a Professor at the University of Saskatchewan College of Law, where she has been a member of faculty since 2005. She holds a law degree from the University of Toronto and a PhD in law from the University of Cambridge. Previously, she has worked at the Supreme Court of Canada, the University of Alberta Health Law Institute and the University of Canterbury School of Law.
Professor von Tigerstrom’s areas of teaching and research are medical law and ethics, public health law and policy, food and drug regulation, and tort law. Her research expertise includes the regulation of pharmaceuticals and legal issues in chronic disease prevention, including policy measures relating to food, alcohol and tobacco. Professor von Tigerstrom is a member of the Canadian Institutes of Health Research (CIHR) Stem Cell Oversight Committee, the Canadian Blood Services Bioethics Advisory Committee and the Law Reform Commission of Saskatchewan.
Dr. Catherine Zahn (Member)
Dr. Zahn was appointed President and CEO of the Centre of Addiction and Mental Health in 2009. Previously, she held senior executive positions at the University Health Network for 12 years.
She received her MD and an MSc in Health Administration from the University of Toronto. Dr. Zahn is a Professor in the U of T faculty of Medicine and a Fellow of the Royal College of Physicians and Surgeons of Canada. She has made numerous contributions to health care through her leadership in hospital integration, technology assessment and mental health-care system improvement.
Honours include membership in the Order of Canada and Doctor of Laws degrees (honoris causa) from Western University and Ryerson University. Dr. Zahn serves on several health and neuroscience related boards and committees. She chairs the Council of Academic Hospitals of Ontario and the Board of the Institute for Clinical Evaluative Sciences.
Annex 2: Terms of Reference
Context
In its December 2015 Speech from the Throne, the Government of Canada reaffirmed its commitment to “legalize, regulate, and restrict access to marijuana”. A commitment has been made to create a new system of strict marijuana sales and distribution, with appropriate federal and provincial sales taxes applied, both to prevent youth from accessing marijuana and to curtail the illegal marijuana market that is benefitting organized crime. A commitment was also made to punish more severely those who provide marijuana to minors, those who operate a motor vehicle while under its influence and those who sell it outside of the new regulatory framework.
To inform the design of a new system, engagement with provinces and territories, as well as key experts, is essential. To carry out this work, the Ministers of Justice and Attorney General of Canada, the Minister of Public Safety and Emergency Preparedness and the Minister of Health (the Ministers) are creating a Task Force on Marijuana Legalization and Regulation (the Task Force).
Purpose
The Task Force will, on the basis of a discussion paper:
- Engage provincial, territorial, and municipal governments, Indigenous governments and representative organizations, youth, and experts in relevant fields, including but not limited to: public health, substance abuse, criminal justice, law enforcement, economics, and industry and those groups with expertise in production, distribution and sales, to seek their views on issues that are fundamental to a legislative and regulatory system for restricted access to marijuana;
- Provide opportunities for all Canadians to provide their input and views on key questions related to the legalization, regulation and restriction of access to marijuana through an online questionnaire and written submissions; and
- Provide a final report to the Government, which will provide advice for the design of a new legislative and regulatory framework for restricted access to marijuana.
Scope
The Task Force will consult on issues fundamental to the design of a new legislative and regulatory system for restricted access to marijuana. A discussion paper, which includes background information and key questions, will provide a starting point for these consultations.
The Task Force’s work will be guided by the following federal objectives:
- Protect young Canadians by keeping marijuana out of the hands of children and youth.
- Keep profits out of the hands of criminals, particularly organized crime.
- Reduce the burdens on police and the justice system associated with simple possession of marijuana offences.
- Prevent Canadians from entering the criminal justice system and receiving criminal records for simple possession of marijuana offences.
- Protect public health and safety by strengthening, where appropriate, laws and enforcement measures that deter and punish more serious marijuana offences, particularly selling and distributing to children and youth, selling outside of the regulatory framework, and operating a motor vehicle while under the influence of marijuana.
- Ensure Canadians are well-informed through sustained and appropriate public health campaigns, and for youth in particular, ensure that risks are understood.
- Establish and enforce a system of strict production, distribution and sales, taking a public health approach, with regulation of quality and safety (e.g., child-proof packaging, warning labels), restriction of access, and application of taxes, with programmatic support for addiction treatment, mental health support and education programs.
- Continue to provide access to quality-controlled marijuana for medical purposes consistent with federal policy and Court decisions.
- Conduct ongoing data collection, including gathering baseline data, to monitor the impact of the new framework.
In carrying out its mandate, the Task Force will be mindful of federal and provincial/territorial jurisdictions.
Public Engagement
In-person sessions
The Task Force will hold targeted face-to-face engagement sessions with key stakeholders across Canada, including:
- Provincial, territorial and municipal governments;
- Experts in relevant fields, including but not limited to: public health, substance abuse, criminal justice, law enforcement, economics, and industry and those groups with expertise in production, distribution and sales;
- Indigenous governments and representative organizations; and
- Youth.
Online consultations
The Task Force will also provide an opportunity for Canadians to provide their views on the key questions related to the legalization, regulation and restriction of access to marijuana through an online consultation portal and/or written submissions.
Timeline
The Task Force will present a final report, which provides advice on the design of a new legislative and regulatory framework, to the Ministers in November 2016. The final report will be made public by the Ministers at a time to be determined by the Ministers.
Annex 3: Acknowledgements
The Task Force would like to recognize the many Canadians, provincial, territorial, and municipal governments, Indigenous governments and representative organizations, youth and experts whose valuable contributions helped to shape the Task Force’s deliberations and Final Report. Individuals who did not meet with the Task Force in person have not been named for privacy reasons.
- Abbotsford Police Department
- ABcann Medicinals Inc.
- Ronald Abrahams – British Columbia Women’s Hospital Association
- Action on Smoking & Health
- Addictions and Mental Health Ontario
- Aerionics, Inc.
- Agro-Greens Natural Products Ltd.
- Alberta 420 – Calgary 420
- Alberta College of Pharmacists
- Alberta Construction Association
- Alberta Urban Municipalities Association
- Alcohol Countermeasure Systems
- Anandia Labs
- Aphelion Pharmaceuticals Inc.
- Arrive Alive DRIVE SOBER
- The Arthritis Society
- Assembly of First Nations
- Association des avocats et avocates de la défense
- Association of Municipalities of Ontario
- Association of Ontario Health Centres
- Association of Yukon Communities
- Association pour la santé publique du Québec
- Association québécoise des intervenants en cannabis médical
- Ateliers Underlabs
- Guillermo R. Aureano – Université de Montréal, Département de science politique
- Aurora Cannabis Inc.
- Avanti Rx Analytics Inc.
- AWLDM
- Gary Barnes – Previous Chairman, Canadian Association of Fire Chiefs
- Gary Bass – Retired Deputy Commissioner, Royal Canadian Mounted Police
- Renaldo Battista – Fonds de recherche du Québec
- B.C. Compassion Club Society
- B.C. Government and Service Employees Union
- B.C. Lung Association
- B.C. Official Opposition
- B.C. Private Liquor Store Association
- Line Beauchesne – University of Ottawa
- Vasiliki Bednar – Rotman School of Business/University of Toronto
- Bedrocan
- Beer Canada
- Billerfy
- Bio Therapeutic Molecules Inc.
- Hilary Black – Founder of the B.C. Compassion Club Society, Bedrocan
- Elder Denise Ann Boissoneau
- Norman Bossé – Child and Youth Advocate for the Province of New Brunswick
- Neil Boyd – Simon Fraser University
- Breakaway Addiction Services
- Serge Brochu – Université de Montréal
- Broken Coast Cannabis
- Thomas Brown – McGill University
- Jeffrey Brubacher – University of British Columbia
- C&B Group
- Calgary Building Services
- Calgary Intergovernmental & Corporate Strategy
- Calgary Police Department
- Canada Medical Cannabis Growers Coop
- Canada’s Building Trades Unions
- Canadian AIDS Society
- Canadian Alliance for Responsible Cannabis Production
- Canadian Association for Pharmacy Distribution Management
- Canadian Association of Chiefs of Police
- Canadian Association of Chiefs of Police Traffic Committee
- Canadian Association of Fire Chiefs
- Canadian Association of Liquor Jurisdictions
- Canadian Association of Medical Cannabis Dispensaries
- Canadian Association of Petroleum Producers
- Canadian Automobile Association
- Canadian Bar Association
- Canadian Cancer Society
- Canadian Cancer Survivor Network
- Canadian Centre for Occupational Health and Safety
- Canadian Centre of Forensic Sciences
- Canadian Centre on Substance Abuse
- Canadian Commercial Growing Solutions
- Canadian Consortium for the Investigation of Cannabinoids
- Canadian Council of Motor Transport Administrators
- Canadian Dental Hygienists Association
- Canadian Don’t Do Drugs Society
- Canadian Drug Policy Coalition
- Canadian Federation of Independent Business
- Canadian Federation of Students
- Canadian Fuels Association
- Canadian Hemp Trade Alliance
- Canadian HIV/AIDS Legal Network
- Canadian Life and Health Insurance Association Inc.
- Canadian Medical Association
- Canadian Medical Cannabis Council
- Canadian Mental Health Association
- Canadian National Medical Marijuana Association
- Canadian Nurses Association
- Canadian Paediatric Society
- Canadian Pharmacists Association
- Canadian Public Health Association
- Canadian Seed Growers’ Association
- Canadian Students for Sensible Drug Policy
- Canadian Therapeutic Cannabis Partners Society
- Canadian Trucking Alliance
- Canadians for Fair Access to Medical Marijuana
- CanEvolve
- Canna Botanicals
- Canna Farms
- Canna Naturals
- Cannabinoid Medical Clinic Ottawa
- Cannabis Access Regulations Study
- Cannabis Canada Association
- Cannabis Conservancy
- The Cannabis Conservancy
- Cannabis Friendly Business Association – www.cannabizassociation.ca
- Cannabis Growers of Canada
- Cannabis Incorporated
- Cannabis Industry Council of Canada
- Cannabis Law & Policy Project
- Cannabis Patients Association of Canada
- Cannabis Skunk Sense
- The Cannabis Trade Alliance of BC
- Cannabis Trade Alliance of Canada
- CannAmm Occupational Testing Services
- Cannevert Therapeutics
- Rielle Capler – University of British Columbia
- Cascade Cultivation Inc.
- Centre for Addiction & Mental Health
- Centre for Addictions Research of B.C.
- Carol Chafe – Child and Youth Advocate for the Province of Newfoundland and Labrador
- Elder Jane Chartrand
- Chief Medical Officers of Health of Canada
- Chiefs of Ontario
- Child and Adolescent Services (Cape Breton Public Health)
- Children and Youth in Challenging Contexts Network
- Chronic Pain Toronto
- Church of the Universe
- City of Calgary
- City of Delta
- City of Duncan Council
- City of Edmonton
- City of Fernie
- City of Langley
- City of Seattle
- City of Toronto
- City of Vancouver
- City of Victoria
- The Hon. Marion L. Cohen – Court of Justice of Ontario
- College of Family Physicians of Canada
- College of Pharmacists for Nova Scotia
- College of Physicians and Surgeons of Alberta
- College of Physicians and Surgeons of Manitoba
- College of Physicians and Surgeons of Ontario
- College of Registered Nurses of Manitoba
- College of Registered Psychiatric Nurses of Manitoba
- Coming Out of the Closet Cannabis Club
- Community Enterprise Network Inc.
- Complementary Healthcare
- Comprehensive Benefit Services Inc.
- Congress of Aboriginal Peoples
- Patricia Conrod – Université de Montréal
- John Conroy
- Construction Labour Relations
- Construction Labour Relations – An Alberta Association
- Construction Labour Relations Association of Saskatchewan Inc.
- Construction Owners Association of Alberta
- Coopérative Cann-Amis
- Corporation of Delta, The
- Darren Courtney – University of Toronto
- Covenant House
- Craft Cannabis Association of British Columbia
- CRCI
- Criminal Lawyers Association
- Kora Debeck – University of British Columbia
- Delisle Youth Services
- Delta 9 Gardening Inc.
- Derivex, BCCannabisLabs, BFS consultant to Licensed Producers
- Direction régionale de santé publique du CIUSSS du Centre-Sud-l’Île-de-Montréal
- Doctors for Cannabis Regulation
- Doctors for Responsible Access
- Doctors Nova Scotia’s Policy and Health Issues Committee
- Dravet.ca
- Drug Free Kids Canada
- Jason Dyck – University of Alberta
- East Coast Seeds
- East Metro Youth Services
- ECS BioMed Inc.
- ECS Safety Services Ltd.
- Edmonton 420 Cannabis Community
- Edmonton Police Services
- Edmonton Stop Marijuana Grow Ops Coalition
- Educators for Sensible Drug Policy
- Irwin Elman – Child and Youth Advocate for the Province of Ontario
- Enform Canada
- Epilepsy Support Centre
- Eurofins Experchem
- Eye Highs Creative Inc.
- Families for Addiction Recovery
- Families for Addiction Recovery and Faces and Voices of Recovery Canada
- Farend Natural Products
- Federal Ombudsman for Victims of Crime
- Federally Regulated Employers – Transportation and Communications
- Fédération des travailleurs et travailleuses du Québec
- Fédération médicale étudiante du Québec
- Federation of Canadian Municipalities
- Federation of Medical Regulatory Authorities of Canada
- First Nations Chiefs of Police Association
- First Nations Health Authority
- Benedikt Fischer – Centre for Addiction & Mental Health
- Foundation of Cannabis Unified Standards
- GalenicaTech Consulting
- Georgian Bay Biomed Inc.
- Glacial Gold
- Good Chemistry
- Good Earth Pharms
- Government of Alberta
- Government of British Columbia
- Government of Manitoba
- Government of New Brunswick
- Government of Newfoundland and Labrador
- Government of Nova Scotia
- Government of Nunavut
- Government of Ontario
- Government of Prince Edward Island
- Government of Saskatchewan
- Government of the Northwest Territories
- Government of the State of Colorado
- Government of the State of Washington
- Government of Uruguay
- Government of Yukon
- Del Graff – Child and Youth Advocate for the Province of Alberta
- Grassroots Cannabis Inc.
- The Green Room Society
- The Green Solution
- Growing Edge Technologies
- GS1 Canada
- Rebecca Haines-Saah – University of Calgary
- Halton Regional Police – Drug and Morality Unit
- David Hammond – University of Waterloo
- Rick Hansen – Retired Chief of Police, Calgary
- Mike Harcourt – Former Premier of B.C.
- Cory Harris – University of Ottawa
- The Hayley Rose Foundation
- Heart and Stroke Foundation
- Heartland Health region
- Horizons Residents
- Horizons Youth
- Hyasynth Bio
- Hydropothecary Inc.
- Elaine Hyshka – University of Alberta
- Indigenous Peoples’ Assembly of Canada
- Injury Free Nova Scotia
- Institute for Behavior and Health, Inc.
- Inter-American Drug Abuse Control Commission
- International Association of Machinists and Aerospace Workers
- International Centre for Science in Drug Policy
- International Ganja Cooperative
- Inuit Tapiriit Kanatami
- Investment Property Owners Association of Nova Scotia
- Emily Jenkins – University of British Columbia
- Justice for Children and Youth
- Didier Jutras Aswad – Centre hospitalier de l’Université de Montréal
- Archie Kaiser – Dalhousie University
- Harold Kalant – University of Toronto
- Kelz Medical Services
- Akwatu Khenti – Dalla Lana School of Public Health/University of Toronto
- Kootenay’s Medicine Tree, The
- La Maison des Jeunes de Jonquière
- Lake Country Brazilian Jiu-Jitsu
- Lakeview Heights Community Association, West Kelowna, BC
- L’Alternative médicinale Ltée
- Le Groupe HEMP.ca
- Let’s Toke Business
- Level the Playing Field Emergency Services
- Lift Cannabis
- Listuguj Mi’gmaq Government, Mi’gmaq Nation
- Raimar Lobenberg – University of Alberta
- The Lung Association – National Office
- MacaqueTV
- Jason MacDougall – Dalhousie University
- Manitoba Centre for Health Policy
- Marijuana Party of Canada
- Marijuana Policy Group
- The Marijuana Victims’ Association Canada
- Marijuana.Ca
- marijuanalaws.ca
- Martin Medical Services
- McCreary Centre Society
- Medical Health Officers of Vancouver Coastal Health
- med-man brand
- MedReleaf
- Mental Health and Addictions with the Nova Scotia Health Authority
- Métis National Council
- Mettrum Ltd.
- Rob Milin – University of Ottawa and Royal Ottawa Hospital
- Mothers Against Drunk Driving Canada
- Mouvement des caisses Desjardins
- National Access Canada Corp.
- National Cannabis Assembly of Canada
- National Drug Prevention Alliance (U.K.)
- National Organization for the Reform of Marijuana Laws Canada
- National Organization for the Reform of Marijuana Laws Women’s Alliance of Canada
- Natural Order Health Services
- Nature’s Way Organics
- Neighbourhood Pharmacy Association of Canada
- New Brunswick Liquor Corporation
- NFC Authority Inc.
- Nomis Holding
- Non-Smokers’ Rights Association
- Northern Health Region – Manitoba
- Nova Scotia Chiefs of Police Association
- Nova Scotia Criminal Lawyers Association
- Ontario Campaign for Action on Tobacco
- Ontario Community Council on Impaired Driving
- Ontario Physical and Health Education Association (Ophea)
- Ontario Provincial Police
- Ontario Public Health Association
- Ontario Public Health Unit Collaboration on Cannabis
- Ontario Public Service Employees Union
- Ontario Tobacco Research Unit, University of Toronto
- Ontario Undergraduate Student Alliance
- Eugene Oscapella – University of Ottawa
- Ottawa Public Health
- Ottawa Public Health – Prevention of Substance Misuse
- Jonathan Page – University of British Columbia
- Palix Foundation
- Pan-Canadian Joint Consortium for School Health
- Parachute, Leaders in Injury Protection
- Parent Action on Drugs
- PatientsFirst.ca
- Peel Public Health
- The Peer Project
- PEI Pharmacist Association
- Peloton Pharmaceuticals
- Pharmacists Manitoba
- Physicians for a Smoke-Free Canada
- Pieces to Pathways
- Pine River Institute
- Portage
- Practitioners for Medicinal Cannabis
- Prairie Plant Systems Inc.
- Private Motor Truck Council of Canada
- Privateer Holdings
- Public Interest Advocacy Centre
- PureLeaf Med
- Rapid Fire Theatre Company
- Dan Reist – University of Victoria
- Responsible Marijuana Retail Alliance of British Columbia
- Retail Council of Canada
- RetroTrust Corporation
- RG Holistics
- River City Genetics
- Robert B. SomervilleCo. Limited
- Sandy Hill Community Health Centre
- Santé Cannabis
- Saskatchewan Human Rights Commission
- The Saskatchewan Medical Cannabis Association
- Saskatchewan Urban Municipalities Association
- Robert Schwartz – University of Toronto
- SeeTek
- Segra Biogenesis Corp.
- Service de police, Agglomération de Longueuil
- Shoppers Drug Mart
- Simon Fraser University Beedie School of Business
- Smart Approaches to Marijuana
- William Smith – Ombudsman for the Province of Nova Scotia
- SneakGuard
- Soma Labs Scientific Inc.
- Eldon Spackman – University of Calgary
- Speekeezy Publication Workshop
- Spirits Canada
- Ste. Anne’s Spa
- Tim Stockwell – University of Victoria
- Stronghold Data Solutions Inc.
- Students Commission of Canada
- SwimJet Inc
- Syndicat des employé(e)s de magasins et de bureaux de la SAQ
- Syro Farms
- Take Back America Campaign
- Tantalus Pharmaceuticals LTD
- TEKSA
- Dr. Philip Tibbo – Dalhousie University
- Tilray
- TLC Consulting
- TomKat Communications
- Toronto Drug Strategy Implementation Panel
- Toronto Police Department
- Toronto Transit Commission
- Kirk Tousaw – Tousaw Law Corporation
- TRACE Youth Cannabis Research Program
- Trellis
- True Leaf Medicine Inc.
- Mary Ellen Turpel-Lafond – Child and Youth Advocate for the Province of British Columbia
- Tweed
- Union of B.C. Municipalities
- University Health Network
- Up! Cafe
- Urban Public Health Network
- Vancouver Aboriginal Friendship Centre Society
- Vancouver Animal Wellness Hospital
- Vancouver Coastal Health Medical Health Officers
- Vancouver Police Department
- Vapelated Vapor Lounge
- Vend Data Media Solutions Canada Inc
- Zach Walsh – University of British Columbia Okanagan
- Waterloo Police Services
- Weedmaps
- Wellington-Dufferin-Guelph Public Health
- Dan Werb – International Centre for Science in Drug Policy
- WMG Logistics
- World Federation Against Drugs
- XeraFlop Technologies
- York Region Public Health
- Yukon Youth Team
- 9519297 Canada Incorporated
The Task Force would also like to recognize the individuals and organizations who hosted meetings:
- Officials from the country of Uruguay, including Diego Olivera, Secretary General of the National Drug Board of Uruguay for organizing a teleconference with the National Drug Board and the Uruguayan Institute for Cannabis’ Control and Regulation as well as the Ministry of Public Health
- Officials in the state of Colorado, including Andrew Freedman – Director of Marijuana Co-ordination, Don Brown – Secretary of Agriculture, Barbara Brohl, Ron Kammerzell, Jim Burack and Lewis Koski from the Marijuana Enforcement Division, who provided advice to the Task Force and organized stakeholder meetings, as well as to the law firm Ireland Stapleton for organizing and hosting a meeting with industry and other stakeholders.
- Rick Garza, Director at the Washington State Liquor and Cannabis Board for his advice and for organizing informative meetings with Washington State officials including officials from the Washington State Liquor and Cannabis Board, the Department of Financial Institutions, Social and Health Services, and the Department of Health, as well as for organizing ride-along visits with enforcement officers to local cannabis stores and licensed producers
- David Mendoza, from the office of the Mayor of Seattle, for organizing a session with city officials including from the City Attorney’s office, the Department of Finance and Administrative Services, the Department of Construction and Inspections and the Seattle Police Department. We also thank the Cannabis Law and Policy Project from the University of Washington School of Law for organizing a meeting with industry and other stakeholders in the state of Washington
- Jenna Valleriani for organizing the Canadian Students for Sensible Drug Policy “Youth Speak: Cannabis Policy in the 21st Century” and the youth who participated
- Youth who participated in the Task Force’s Youth Roundtable:
- Kwaku Agyemang,
- Karly Church,
- Kodiak Glennie,
- Chataya Holy Singer,
- Tiffany Kummer,
- Adalia Neibergall,
- Rebecca Singbeil, and
- Brandon Timmerman.
- The Arthritis Society, Canadians for Fair Access to Medical Marijuana, Canadian AIDS Society and Hilary Black for organizing a meeting with medical cannabis patients, and to those who participated:
- Ron Allison,
- Leslie Best,
- Mary Brachaniec,
- Daphnée Elisma,
- Jordan G.,
- Scott Henderson,
- Jules Howllett,
- Ljubica Kostovic,
- Gerald Major,
- Enrico Mandarino,
- Shari Margolese,
- Mandy McKnight,
- Garry Mellan, and
- Dwight Villeneuve.
The Task Force would also like to extend its appreciation to Beau Kilmer and Steve Rolles for their counsel and advice.
Annex 4: Discussion Paper ‘Toward the Legalization, Regulation and Restriction of Access to Marijuana’
A. Introduction
In the 2015 Speech from the Throne, the Government of Canada committed to legalizing, regulating, and restricting access to marijuana.
The current approach to marijuana prohibition is not working:
- Youth continue to use marijuana at rates among the highest in the world.
- Thousands of Canadians end up with criminal records for non-violent drug offences each year.
- Organized crime reaps billions of dollars in profits from its sale.
- Most Canadians no longer believe that simple marijuana possession should be subject to harsh criminal sanctions, and support the Government’s commitment to legalize, tax and regulate marijuana.
The Government understands the complexity of this challenge and the need to take the time to get it right.
The Minister of Justice and Attorney General of Canada, supported by the Minister of Public Safety and Emergency Preparedness and the Minister of Health, has created a Task Force on Marijuana Legalization and Regulation (“the Task Force”). The Task Force is mandated to engage with provincial, territorial and municipal governments, Indigenous governments and representative organizations, youth, and experts in relevant fields, including but not limited to: public health, substance abuse, criminal justice, law enforcement, economics, and industry and those groups with expertise in production, distribution and sales. The Task Force will provide advice on the design of a new framework. The Task Force will receive submissions from interested parties, including individual Canadians, consult widely, listen and learn, and commission any necessary focussed research to support its work. It is supported by a federal secretariat and will report back to the three Ministers on behalf of the Government in November 2016, on a date to be determined by the Ministers.
This Discussion Paper is designed to support consultations led by the Task Force. Its goal is to support a focussed dialogue.
Objectives
The Government of Canada believes that the new regime for legal access to marijuana must achieve the following objectives:
- Protect young Canadians by keeping marijuana out of the hands of children and youth.
- Keep profits out of the hands of criminals, particularly organized crime.
- Reduce the burdens on police and the justice system associated with simple possession of marijuana offences.
- Prevent Canadians from entering the criminal justice system and receiving criminal records for simple marijuana possession offences.
- Protect public health and safety by strengthening, where appropriate, laws and enforcement measures that deter and punish more serious marijuana offences, particularly selling and distributing to children and youth, selling outside of the regulatory framework, and operating a motor vehicle while under the influence of marijuana.
- Ensure Canadians are well-informed through sustained and appropriate public health campaigns, and for youth in particular, ensure that risks are understood.
- Establish and enforce a system of strict production, distribution and sales, taking a public health approach, with regulation of quality and safety (e.g., child-proof packaging, warning labels), restriction of access, and application of taxes, with programmatic support for addiction treatment, mental health support and education programs.
- Continue to provide access to quality-controlled marijuana for medical purposes consistent with federal policy and Court decisions.
- Conduct ongoing data collection, including gathering baseline data, to monitor the impact of the new framework.
B. Background
A brief overview of marijuana
The cannabis plant is found throughout the world, but has its origins in Asia. It has been used for millennia for its psychoactive effects–euphoria (“the high”), relaxation, a sense of well-being, and intensification of ordinary sensory experiences (i.e., sight, sound, taste, smell). However, it has also historically been used for medical and social purposes.
A variety of products can be produced or derived from the flower of the cannabis plant including:
- dried herbal material (i.e., “marijuana”);
- oil (e.g., “hash oil”);
- hash (i.e., compressed resin);
- concentrates (e.g., “shatter”); or,
- foods and beverages containing extracts of cannabis.
Cannabis is most often smoked (as a dried herbal product, either alone or as a concentrate mixed with tobacco), but it can also be vaporized, or eaten.
Cannabis contains hundreds of chemical substances, among which are over 100 known as “cannabinoids.” Cannabinoids are a class of chemical compounds that act on receptors in cells in the brain and body. The most well-studied cannabinoid is THC (tetrahydrocannabinol), the primary psychoactive compound of cannabis (i.e., the chemical responsible for the “high”). Increasing attention is also being paid to another key cannabinoid–CBD (cannabidiol). Unlike THC, CBD is not psychoactive and may in fact counteract some of the psychoactive effects of THC. There is increasing scientific study into the potential therapeutic uses of CBD.
For the purposes of this discussion paper, the popular term “marijuana” is used throughout, unless a specific reference to a marijuana derivative product is being made.
Prevalence of use
Marijuana is the world’s most used illicit psychoactive substance. Estimates from the United Nations Office on Drugs and Crime (UNODC) suggest that around 200 million people globally reported using marijuana at least once in 2012. A UNICEF report published in 2013 ranked Canada highest amongst all nations in terms of rates of marijuana use among youth.
Marijuana has been prohibited in Canada since the 1920s and is listed as a controlled substance in Schedule II of the Controlled Drugs and Substances Act(CDSA). As a result, possession, production and trafficking of marijuana are illegal. The Marihuana for Medical Purposes Regulations (MMPR)provide a regime allowing for legal access to marijuana for medical purposes.
Despite these prohibitions, marijuana remains the most commonly used illicit substance in Canada. It is the second most used recreational drug in Canada after alcohol, especially among youth. An estimated 22 million Canadians 15 years of age and older, approximately 75% of the population, drank alcohol in 2013. In contrast, eleven per cent of Canadians aged 15 or older reported having used marijuana at least once in 2013. When examined more closely, the data reveals that 8% of adults over the age of 25 reported past-year use of marijuana in 2013, whereas 25% of youth aged 15-24 reported past-year use.
The criminal justice system
Marijuana is the most trafficked drug in the world. In Canada alone the illegal trade of marijuana reaps an estimated $7 billion in income annually for organized crime. In addition, the https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistrative burden and social harms associated with the enforcement of marijuana laws, particularly for simple possession, are onerous, and need to be balanced with other safety priorities. Some Canadians argue that these laws are disproportionate to the seriousness of marijuana use as a criminal offence.
The current approach also creates challenges for the criminal justice system and for Canadians. Significant resources are required to prosecute simple possession offences. In 2014, marijuana possession offences accounted for 57,314 police-reported drug offences under the CDSA; this is more than half of police-reported drug offences. Of these, 22,223 resulted in a charge for possession that year.
The criminal records that result from these charges have serious implications for the individuals involved. People with criminal records may have difficulty finding employment and housing, and may be prevented from travelling outside of Canada. On a larger scale, criminal justice system resources are required to address the involvement of organized crime in the illicit marijuana market. In 2015, the Criminal Intelligence Service Canada reported 657 organized crime groups operating in Canada, of which over half are known or suspected to be involved in the illicit marijuana market.
The link between organized crime and the illicit marijuana market is well established. Due to the popularity of the drug among the general public, profitability, and the relative ease of production and cultivation, several significant Canadian-based organized crime groups and networks are involved in the production and distribution of marijuana. The majority of marijuana in the Canadian illicit market is believed to be produced domestically. In 2013, Health Canada reported that Canadian law enforcement sought destruction for over 39 metric tonnes of dried marijuana and more than 800,000 marijuana plants. As well, illicit marijuana grow operations exist in all parts of Canada and in all types of communities. Marijuana also moves across our borders, and according to the Canada Border Services Agency, between 2007 and 2012 marijuana was one of the top three types of drugs involved in drug seizure operations.
Police and the court system must also deal with individuals who drive while impaired by marijuana. In 2013, 97% of police-reported impaired driving incidents involved alcohol and 3% involved drugs (including marijuana), an increase from the reported 2% in 2011.
The Canadian Centre on Substance Abuse estimated that, based on 2002 data, public costs associated with the https://e4njohordzs.exactdn.com/wp-content/uploads/2021/10/tnw8sVO3j-2.pngistration of justice for illicit drug use (including police, prosecutors, courts, correctional services) amounted to approximately $2.3 billion annually.
Health effects
There are both health risks and potential therapeutic benefits from marijuana. Most of the research on marijuana over the past five decades has focused on harms, with much less attention placed on potential therapeutic benefits. The illegal status of marijuana has made it difficult to draw a complete picture of the harms of its use compared to those associated with alcohol or tobacco use, or other psychoactive substances. The following summary is based on the current available evidence.
Health risks
In general, health risks associated with marijuana use can be acute (i.e., immediate and short-lived) or chronic (i.e., delayed and longer-lasting). However, the risks may increase significantly depending on a number of factors, including:
- age at which use begins;
- frequency of use;
- duration of use;
- amount used and potency of the product;
- a user’s actions while intoxicated, such as driving or consuming other substances or medications; and,
- a user’s health status and medical, personal, and family health history.
More specifically:
- Frequency of use: Daily or near-daily use of marijuana can have serious long-term effects on a user’s health, including risk of addiction, earlier onset or worsening of some mental illnesses in vulnerable individuals, and difficulty thinking, learning, remembering, and making decisions. Such effects may take days, weeks, months or years to resolve after use is stopped, depending on how long one has been using and when use began. Regular smoking can also harm the lungs.
- Age at which use begins: Health risks associated with marijuana use during adolescence and young adulthood, when brains are still developing, can have greater long-term harm than use during adulthood. This can include the potential for addiction, long-lasting negative effects on proper cognitive and intellectual development, harms to mental health, poor educational outcomes, and reduced life satisfaction and achievement. There is good evidence that regular marijuana use that begins in early adolescence can harm scholastic achievement, and increase the risk of dropping out of school.
- Individual health status: Besides youth, other people who are more vulnerable to the risks and harms of marijuana include those with a history of drug abuse/addiction, childhood abuse, trauma or neglect, people with certain mental illnesses and mood disorders, and children whose mothers used marijuana during pregnancy. Early and regular marijuana use has been associated with an increased risk of psychosis and schizophrenia, especially in those who have a personal or family history of such mental illnesses. In individuals with a history of psychiatric illness, use of marijuana can worsen the illness and complicate treatment.
Perception of risk
Despite increased risks for adolescents who use marijuana, the 2015 Ontario Student Drug Use and Health Survey reported that, among adolescents, the perceived risk of harm associated with marijuana use is actually decreasing. Others have observed that there is an inverse relationship between perception of risk and actual use (i.e., use of marijuana would go up as more people perceive it to be low risk).
Comparison with other psychoactive substances
The illegal status of marijuana makes it difficult to draw a complete picture of the harms of marijuana use compared to those associated with alcohol, tobacco or other psychoactive substances. The most well-established long term harm of regular marijuana use is addiction. Nevertheless, based on what is currently known, the risk of marijuana addiction is lower than the risk of addiction to alcohol, tobacco or opioids. And, unlike substances such as alcohol or opioids where overdoses may be fatal, a marijuana overdose is not fatal.
The “gateway” theory
Marijuana has often been dubbed the “gateway drug”– a stop on the way to the use of more harmful drugs and more serious drug addiction.
The so-called “gateway hypothesis” was popular in the 1970s/80s and neatly described a specific, progressive and hierarchical sequence of stages of drug use that begins with the use of a “softer drug” (e.g., marijuana) and escalates to use of “harder drugs” (e.g., cocaine).
However, over the years, many exceptions to and problems with the “gateway hypothesis” have surfaced. Because of this, the validity and relevance of this hypothesis have been challenged. There is now evidence that suggests that complex interactions among various individual/ predisposing factors and environmental factors (e.g., peer-pressure, family influence, drug availability, opportunities for drug use) drive drug seeking, drug use/abuse, and drug addiction, and these interactions are not necessarily tied to marijuana use alone.
Therapeutic benefits
With respect to claims of marijuana’s therapeutic benefits, aside from clinical studies with marijuana-derived products that have received market authorization in Canada (i.e., dronabinol/Marinol®, nabilone/Cesamet®, nabiximols/Sativex®), only a limited amount of credible clinical evidence exists.
Some clinical studies suggest that strains containing mainly THC have potential therapeutic benefits for some medical conditions, including:
- severe nausea and vomiting associated with chemotherapy;
- poor appetite and significant weight loss as a result of serious long-term or terminal disease (e.g., cancer, HIV/AIDS);
- certain types of severe chronic pain (e.g., neuropathic);
- symptoms associated with inflammatory bowel disease;
- insomnia and anxiety/depression associated with serious long-term disease;
- muscle spasms associated with multiple sclerosis; and,
- symptoms encountered in palliative care settings.
Emerging evidence also suggests that marijuana strains containing mainly CBD may be useful in treating treatment-resistant epilepsy in children and adults.
Global context and International Obligations
Canada is party to the three major United Nations (UN) Conventions on narcotic drugs. In the context of the Convention, Canada is obliged to criminalize the production, sale and possession of cannabis for non-medical and non-scientific purposes. Legalization of marijuana is not in keeping with the expressed purposes of the drug conventions.
While illegal in most countries, the approach to marijuana is shifting in some jurisdictions. Twenty-two countries have adopted some form of decriminalization (decriminalizing marijuana means that it is still illegal but criminal sanctions have been replaced by fines or other types of penalties. This is a separate concept from legalization). This decriminalization has taken effect either in law or through policies, guidelines and/or enforcement discretion. Decriminalization is viewed, by most observers, as consistent with the drug conventions, particularly where it involves personal consumption of small amounts of “soft drugs”.
Despite this emerging shift globally in approaches to controlling and minimizing harms associated with marijuana use, Uruguay remains the only country that has fully legalized marijuana to date.
At a federal level, the United States’ government continues to express opposition to the legalization of marijuana and it remains illegal in federal law. However, the question of legalizing marijuana use is increasingly being posed by State legislators, despite the fact that it remains illegal under federal law. Currently, four States as well as the District of Columbia have legalized access to marijuana, and several more States will vote on similar propositions in 2016 and 2017. Lessons learned from the recent experiences of the states of Colorado and Washington, and from Uruguay, can be useful when considering the new system for Canada.
Some of the key lessons learned that have been reported from the Colorado and Washington State experiences include:
- Identify clear and measurable objectives;
- Develop a comprehensive regulatory system that controls product formats; that prevents commercialization through advertising controls; and that prevents use by youth;
- Allow for effective implementation by:
- taking the time needed for an effective launch;
- developing clear and comprehensive public communications;
- establishing a strong evidence base and data collection strategy to enable long-term monitoring and adjustments to meet policy objectives; and,
- undertaking public health education before legalization begins.
When contemplating changes to the illegal status of marijuana, countries must also give due consideration to the rule of law and to their obligations under the UN conventions.
This dynamic international environment requires that consultations occur with the global community as Canada moves toward the legalization of marijuana, including with the International Narcotics Control Board (INCB) and the United States. While Canada’s proposal to legalize marijuana may differ from drug control policy in other countries, it shares the objectives of protecting citizens, particularly youth; implementing evidence-based policy; and putting health and welfare at the centre of a balanced approach to treaty implementation. Canada is committed to respecting international partners and to seeking common ground in pursuit of these objectives.
C. Discussion issues: elements of a new system
In establishing a new regime for the legalization, regulation and restriction of access to marijuana, several of the regime’s elements are largely self-evident:
- Legalization of the possession of a certain quantity of marijuana obtained within a regulated legal framework, thereby addressing concerns about criminal records and burdens on the justice system for simple possession offences.
- Establishment of a strict, well-regulated system for the production and distribution of marijuana, thereby addressing concerns about the quality, safety and potency of marijuana legally available, and the control of access for those eligible to possess it.
- Continued enforcement of laws and sanctions against possession, production, and distribution of marijuana outside the regulated legal framework.
- Support for prevention and education activities, addictions treatment, counselling, law enforcement and other services to deal with the negative aspects of marijuana use and abuse.
- Education and awareness activities to ensure the risks of marijuana are known, particularly to youth.
- Baseline data and ongoing surveillance and research activities to monitor and evaluate the impact of the new framework.
However, the design and implementation of a new regime will also require careful attention to a number of particularly challenging issues which can be grouped into five themes. The Government is seeking advice and input from experts and stakeholders as well as individual Canadians in these areas:
- Minimizing harms of use.
- Establishing a safe and responsible production system
- Designing an appropriate distribution system.
- Enforcing public safety and protection.
- Accessing marijuana for medical purposes.
The discussion below sets out for each of these five themes:
- Considerations: A synopsis of pertinent facts, concepts and factors that will shape and influence the new regime.
- Possible Options: Key potential elements and provisions of the new regime to achieve the desired objectives.
- Questions: Specific issues and concerns on which the Task Force is seeking ideas and input from provinces, territories, experts, stakeholder groups and the broader public.
1. Minimizing harms of use
Considerations
One of the central issues to consider in the design of a legal and regulatory framework for legal access to marijuana is to identify those system features that will best reduce the risks of health and social harms associated with use.
When considering how best to minimize harms associated with marijuana use, it is helpful to consider the two different approaches taken in controlling tobacco and alcohol use.
In the case of tobacco, the overall objective is to reduce or even eliminate use for all Canadians.
In contrast, the overall objective with respect to alcohol is to promote responsible use amongst adults, and to prohibit use amongst youth. These objectives are achieved largely through actions such as setting a minimum age for purchase, educational tools aimed at promoting responsible use, and taxation measures.
Given that the majority of harms related to marijuana use appear to occur in select high-risk users (e.g., youth) or in conjunction with high-risk use practices (e.g., frequent use; highly potent products; impaired driving), an approach that draws lessons from both tobacco and alcohol control should be examined. Both approaches rely on a comprehensive suite of actions aimed at those users at highest risk for harms through active prevention, education and treatment, as well as policy and legislative interventions.
Few other countries have been as successful as Canada in lowering smoking rates and shifting public attitudes about tobacco. Canadian smoking rates are among the lowest in the world, dropping from 22% in 2001 to 15% in 2013. Since 2001, actions taken under the Government of Canada’s Federal Tobacco Control Strategy have helped lay the foundation for continued success in tobacco control. Such actions include:
- restrictions on tobacco advertising;
- mandatory health warning messages on tobacco packaging;
- minimum age for legal purchase of tobacco;
- public health education campaigns against smoking; and,
- excise tax changes to make tobacco less affordable and accessible.
In addition, all provinces and territories have tobacco legislation of their own. Many municipalities have also taken action in their sphere. This collective action has helped drive the rate of tobacco use among Canadian youth aged 15–17 to its current low of 7%. Another key measure underpinning the success of Canada’s tobacco control efforts has been the way smoking has become socially unacceptable, or “denormalized”, particularly among youth.
In contrast, alcohol consumption is highly normalized in Canadian society, with nearly 75% of adult Canadians reporting that they have used alcohol in the previous year. In part this may be explained by the different regulatory and other control measures that have been implemented. For example, alcohol remains heavily marketed and promoted to adults.
When examining the current frameworks for tobacco and alcohol control, it is also worth noting the different approaches to regulating taken at the federal level. In the case of tobacco, the Tobacco Act protects the health of Canadians by imposing certain minimum standards, such as quantities to be sold in packages, prohibitions on flavours that appeal to youth, and restricting the age of purchase. In contrast, with alcohol, there are no comparable national minimum standards set and federal regulatory oversight is mainly focused on labelling requirements.
These two examples highlight different regulatory approaches and point to the potential for regulation of the same product by different orders of government.
The early experiences of Colorado and Washington State suggest very strongly that the Government should take steps to avoid the commercialization of legalized marijuana, including the active promoting and marketing of marijuana, leading to widespread use. Preventing widespread use–or “normalization”–is especially important when considering the need to decrease rates of use amongst Canadian youth. Marijuana is not a benign substance and the scientific evidence clearly demonstrates that young people are at a higher level of risk for experiencing negative impacts. Protecting youth and children from the negative consequences of marijuana use is central to the Government’s interest in legalizing, regulating and restricting access.
As with the experience in tobacco and alcohol control, the need for a comprehensive approach to prevention, education, and treatment is clear, including public education strategies aimed at better informing youth and families of the risks and harms, in tandem with a range of other safeguards that are described below.
Possible Options
It is proposed that establishing a national minimum standard for protecting Canadians is critical, and as such it is proposed that federal legislation and regulation be developed to create an overall framework for legal access to marijuana. This framework would address the following issues:
- Minimum age for legal purchase: Health protection–particularly for children and youth–demands that marijuana purchase and possession be subject to age restrictions. The science indicates that risks from marijuana usage are elevated until the brain fully matures (i.e., when someone reaches about age 25). For context, age limits for alcohol and tobacco purchases in Canada vary across provinces and territories–either 18 or 19 years of age. In Colorado and Washington, the state governments have chosen to align the minimum age for purchasing marijuana with the minimum age for purchasing alcohol, 21 years.
- Advertising and marketing restrictions to minimize the profile and attractiveness of products: Since marketing, advertising and promotion of marijuana would only serve to “normalize” it in society and encourage and increase usage, it has been proposed that these should be strictly limited so as to dampen widespread use and reduce associated harms. This is particularly the case for promotional materials that would otherwise be targeted to impressionable youth. As in the case of tobacco, there may be limitations to possible restrictions on marketing, advertising and promotion of marijuana; however within those limits these restrictions should be as tight as possible. Moreover, other limitations could include products being sold in plain packaging with appropriate health warning messages.
- Taxation and pricing: When used appropriately, effective taxation and price controls can discourage the use of marijuana and provide the government with revenues to offset related costs (such as substance abuse services, law enforcement, and regulatory oversight). As such, the design of any regulatory framework should allow accommodation for an appropriate taxation regime in which there is sufficient flexibility in controlling the final price to the consumer. However, the use of taxation and pricing measures to discourage consumption must be properly balanced against the need to minimize the attractiveness of the black market and dissuade illegal production and trafficking.
- Limits of allowable THC potency in marijuana: THC is the main psychoactive component of marijuana. Current research shows average THC levels of between 12-15%. In contrast, marijuana from the 1980s had average THC levels of 3%. In addition, various higher potency marijuana products such as “shatter” are available with THC concentrations reaching levels as high as 80-90%. As outlined in section 1, higher concentration products have added risks and unknown long term impacts, and those risks are exacerbated for young people, including children. Given the significant health risks, maximum THC limits could be set and high-potency products strictly prohibited.
- Restrictions on marijuana products: Marijuana can be consumed in many ways, including a wide range of products like foods, candies, salves or creams. Some people may choose these methods of consumption, rather than choosing to smoke dried marijuana. However, certain products present increased risks, notably when considering the increased potency of some of these derivative products and the increased harms associated with their use. They also represent an increased risk of accidental or unintentional ingestion, particularly by children. This view is supported by the experience in Colorado, where the availability of edible products led to a rise in the number of accidental or unintentional overdoses (non-fatal). As a result, the state government amended their regulatory framework to enact limits on dosing and potency. It is understood that individuals may choose to create marijuana products, such as baked goods, for personal consumption. However, consideration should be given to how edibles are treated in the new regime in light of the significant health risks, particularly to children and to youth, including whether and how to limit the potency of marijuana and types of products sold.
- Limitations on quantities for personal possession: Most jurisdictions have set limits on the quantities of marijuana that an individual may possess, which has the obvious advantages of helping to dampen demand and to minimize opportunities for resale of legally purchased marijuana on the illicit market (particularly to children and youth).
- Limitation on where marijuana can be sold: The availability of marijuana via retail distribution is also an important issue when considering means to minimize harms of use. This issue is further explored in Section 3.
Questions
- Do you believe that these measures are appropriate to achieve the overarching objectives to minimize harms, and in particular to protect children and youth? Are there other actions which the Government should consider enacting alongside these measures?
- What are your views on the minimum age for purchasing and possessing marijuana? Should the minimum age be consistent across Canada, or is it acceptable that there be variation amongst provinces and territories?
2. Establishing a safe and responsible production system
Considerations
Important lessons can be learned from Canada’s experience with the production of marijuana for medical purposes in terms of establishing a safe and responsible production system. Legal access to marijuana for those with a medical need began in the late 1990s in response to an Ontario court decision. This and a series of subsequent decisions confirmed Canadians’ constitutional right to reasonable access to a legal source of supply of marijuana for medical purposes. The program and regulatory framework evolved based on these court decisions.
Three main production models have been used either alone or in combination: home cultivation, government-contracted production, and a competitive market model of licensed producers.
Under the former home cultivation regime, the number of Canadians authorized to consume marijuana rose exponentially to approximately 40,000 from less than 500 over the period 2002 to 2014. As the amount of marijuana authorized grew to an average of 18 grams per day, translating into an average of nearly 90 plants, problems with the regime emerged. Issues included increased risks to the occupants from mould, pesticides, fire and increased risk of home invasion. Neighbours and landlords were also affected, as were local services called upon to deal with issues arising from home grow. It was also virtually impossible for Health Canada inspectors to provide effective oversight of home grow operations for two main reasons: the large number of locations spread across the country, and the inability of inspectors to enter a private residence without either permission from the occupant or a warrant.
Likewise, government-contracted production had significant limitations. Health Canada contracted for the production of a certain amount of marijuana grown to specified quality standards, which was then made available for purchase to medically authorized individuals. Fewer than 10% chose to buy this product. Issues included: a lack of variety of choice of type and strain; and concerns by some about price. In addition, the price paid for the marijuana did not fully cover the cost, resulting in significant taxpayer subsidization.
The current model, the Marihuana for Medical Purposes Regulations (MMPR), is exclusively a regulated competitive model. Under the MMPR, as of June 28, 2016, there were 33 licensed producers, 416 applications in the queue, and approximately 20 new applications being received each month. Moving forward, this type of regime with competitive market forces could be one model for production of marijuana. It has a variety of potential advantages including making available a wide variety of strains at different prices.
In addition to this regulated but largely market-driven competitive model, there are other options that could be explored, some of which would involve greater government management of the market. For example, a competitive auction system where qualified applicants pay for the right to operate could be considered. This approach is similar to how the Government of Canada sells government securities. Another model would require the Government to estimate the size of the market, determine how many producers can serve that market, and issue licenses accordingly (similar to the approach used in Washington State).
Several jurisdictions have legalized marijuana for recreational purposes – including Uruguay and, in the U.S., Colorado, Alaska, Oregon, Washington and the District of Columbia. With the exception of the District of Columbia, these jurisdictions allow for the production of marijuana through licensed commercial growers. In addition, all except for Washington permit individuals to grow their own marijuana. All of these jurisdictions place restrictions on the number of plants that individuals can grow. In the U.S., Colorado, Alaska and the District of Columbia allow their citizens to grow a maximum of six plants. Uruguay also permits the cultivation of up to six plants. Oregon allows its residents to grow four plants.
A key principle for consideration common to all models is whether those growing marijuana should have to pay a licensing fee so that taxpayers are not required to subsidize the full cost of government oversight of the program.
Regardless of the production model selected, a new regulatory framework for legal marijuana could contain features designed to ensure good manufacturing practices in a safe and secure environment. This could help to address both the potential health risks from marijuana as well as the need to ensure that marijuana produced in the legal framework stays in the legal framework. The marijuana could be subject to appropriate testing, packaging and labelling requirements both to protect children and to ensure adult users have the necessary information to make informed choices. The MMPR contain these features and could serve as a reference point for consideration of the nature and extent of the safeguards required in the legal marijuana regime.
Possible Options
- Production Model: Experience with both home cultivation and government-controlled production in the context of relatively small numbers of medical users suggests neither approach would be in the public interest in the context of the larger numbers of users expected in a legalized market. Therefore, some form of private sector production with appropriate government licensing and oversight could allow for safe and secure production of legal marijuana with adequate choice (both price and strain) for consumers.
- Good production practices: In general, ingestible products must meet certain quality standards. In the medical marijuana regime, Health Canada has established product content and production controls that have proven effective in minimizing risks to clients. Similarly, safeguards could be put in place to ensure that marijuana is produced and stored in sanitary and secure conditions. There could be strict security requirements to minimize the possibility of diversion. Controls could be placed on pesticides that can be used, and on microbial and chemical contaminants. Marijuana could also be subject to analytical testing so that those consuming can be reliably advised of its contents, particularly amounts of THC and CBD.
- Product packaging and labelling: The way in which products are packaged and labelled offers an opportunity to minimize the harms of marijuana, particularly for children and youth. Measures to consider implementing include: child-proof packaging to prevent accidental ingestion by children; and, labels on packages to contain both important information about the product (e.g., THC and CBD content) as well as appropriate health warning messages.
Questions
- What are your views on the most appropriate production model? Which production model would best meet consumer demand while ensuring that public health and safety objectives are achievable? What level and type of regulation is needed for producers?
- To what extent, if any, should home cultivation be allowed in a legalized system? What, if any, government oversight should be put in place?
- Should a system of licensing or other fees be introduced?
- The MMPR set out rigorous requirements over the production, packaging, storage and distribution of marijuana. Are these types of requirements appropriate for the new system? Are there features that you would add, or remove?
- What role, if any, should existing licensed producers under the MMPR have in the new system (either in the interim or the long-term)?
3. Designing an appropriate distribution system
Considerations
In Canada the only legal marijuana sales take place by licensed producers and they are restricted to using the mail. This provides reliable, low cost delivery to all parts of the country in a discrete manner that does not encourage increased usage. It also helps keep prices low as no overhead is required to maintain a retail distribution system. However, illegal sales in Canada also occur in a variety of ways including through store-fronts (“dispensaries”) and over the internet.
Legal sales in other jurisdictions occur through a variety of means. For instance, in Colorado, the law allows for cities and counties to decide if they will permit recreational stores. To date, over 300 stores have been established, selling dried marijuana and a range of edible and other products. In Washington, the state is issuing a specified number of licenses for the legal operations of dispensaries.
In both Colorado and Washington, public consumption is not allowed. To address consumption in public, some jurisdictions, such as Uruguay and Holland, allow venues for the legal consumption of marijuana, such as “coffee shops” or clubs.
As discussed in Section 1, perceptions around the risk of a substance and its “normalcy” in society can affect levels of usage. The choice of a distribution system can impact these perceptions and thus may ultimately have an effect on usage rates. The distribution model could also have more direct consequences for health and safety. For example, in recognition of the more serious impairment that results when alcohol and marijuana use are combined, both Washington and Colorado do not allow marijuana to be sold in stores that also sell alcohol. Finally, different delivery models carry different considerations e.g., ability to prevent sales to minors, access in remote locations, local tax base, ability to distinguish between sales of legally produced marijuana from illicit product, and so on.
Possible Options
- Phased-in approach to distribution: In the initial stages of legalizing marijuana, only allowing a proven system of distribution (e.g., through the mail, as is currently done in the medical marijuana regime) could minimize the risks of uncontrolled/illegal retail sales outlined above. This system could enable access for adults while using caution in taking a step that may inadvertently put youth at increased risk.
- Storefronts: On the other hand, allowing for some ability for the sale of marijuana to occur in a legal, regulated retail environment may be required in order to provide an alternative to the current illegal sellers that exist in certain Canadian cities. Ensuring that the marijuana sold in such establishments comes from a legal source would be critical.
- Local choice: Alternatively, decisions on appropriate distribution mechanisms could be left to provincial and territorial governments to determine the best approach based on their unique circumstances. This scenario could result in different models being adopted across the country.
Regardless of the distribution model ultimately chosen, significant efforts by all orders of government and by law enforcement will need to be put into shutting down illegal operations, be they store-fronts or internet operators. See section 4 for more discussion on this point.
Questions
- Which distribution model makes the most sense and why?
- To what extent is variation across provinces and territories in terms of distribution models acceptable?
- Are there other models worthy of consideration?
4. Enforcing public safety and protection
Considerations
Establishing a successful legalization regime will require a clear and robust legislative and regulatory framework. Law enforcement will also need to explore their role, and develop policy, training and practices. This will need to be coupled with appropriate actions to enforce measures outlined in the new regime and to deal with those who operate outside of it if the objectives detailed earlier in this paper are to be achieved.
As the experiences of other jurisdictions and of the regulation of alcohol and tobacco in Canada have shown, regulating a substance does not automatically remove it from illicit markets (e.g., contraband tobacco). In fact, experiences to date in Colorado confirm the need for consistent enforcement of regulations, and investing in the development of new policies, training and tools for those responsible for enforcement. Among other objectives, this can help to prevent and address impaired driving and diversion to youth, control the black market, and deal with associated crimes.
In designing the new system for legal access, close consideration must be given to new or strengthened sanctions for those who act outside the boundaries of the new system. For example, new laws may be necessary to punish those who sell to minors. Also, vigilant enforcement as well as new or strengthened laws, at the federal, provincial or territorial, or local level, may be needed to consistently protect public and individual health and safety by addressing:
- concerns regarding the location of production or distribution sites;
- hours of operation;
- density or overall number of producers and/or retailers; and,
- consumption of marijuana outside of personal dwellings (e.g., public space).
The law enforcement community will be responsible for enforcing the laws that support the new regime. If the regime (e.g., production, distribution, taxation, consumer access, etc.) is too complex or onerous for enforcement and legal production and access, there will be opportunities for organized crime to satisfy the demand through the illicit market.
While one of the objectives of legalization is to keep profits out of the hands of criminals, organized crime groups and networks currently entrenched in the Canadian illicit marijuana market may continue to produce and distribute marijuana outside of the new regime if there is profit to be made. There may be risk of theft and the diversion of marijuana from the legitimate supply chain. There are a number of other scenarios and challenges related to organized crime that will need to be minimized in a legalized system. Discussions with key law enforcement stakeholders will be essential.
Another central objective is the need to guard against marijuana-impaired driving. Driving while impaired by alcohol and/or drugs, including marijuana, is an offence under the Criminal Code of Canada. Impaired driving continues to kill and injure more Canadians than any other crime.
Marijuana impairs a number of brain functions needed for safe driving such as co-ordination, judgment of distances, reaction time, and ability to pay attention. Marijuana is second to alcohol as the drug most frequently found among drivers involved in crashes and drivers charged with impaired driving, and among seriously injured drivers. Marijuana and alcohol are also among the most frequently occurring alcohol-drug combinations.
In contrast to alcohol, there is currently no roadside “breathalyzer”-type test to detect impairment with marijuana. However, roadside oral fluid tests are being used in other jurisdictions that can detect the presence of marijuana in oral fluid which can be suggestive of recent use. This is an active area of Canadian and international research.
The development of tools, training and forensic laboratory capacity would be required for the Canadian law enforcement community to mitigate any potential increase in drug-impaired driving related to legalization of marijuana. For example, the government could establish an offence of driving while having a specified concentration of THC in the blood, similar to the offence of driving with a blood alcohol level at or above the legal limit and/or it could authorize roadside oral fluid screening devices for THC.
Possible Options
- Strengthened laws and appropriate enforcement response: Establishing a successful legalization regime will require the strengthening of laws that will minimize or eliminate criminal involvement. It could also require the strengthening of laws to punish those who choose to operate outside of its parameters, including those who provide marijuana to youth or produce or traffic marijuana outside of the new regulated framework, and move it across Canadian borders.
- Enforcement tools for marijuana-impaired driving: There is a need and opportunity for Canada to research, develop, test, train and promote technologies and related guidelines and protocols that can equip law enforcement to deal with possible increased rates of impaired driving, particularly for roadside testing of impairment. This should be complemented by public education campaigns that emphasize risks associated with drug-impaired driving and that advocate preventive measures, as is the case for drinking and driving.
- Restriction of consumption to the home or a limited number of well-regulated publicly-accessible sites: Consumption of marijuana could be restricted to private residences. However, the system may need to be pragmatic to respond to the demand for venues to consume marijuana outside the home in order to avoid proliferation of consumption in all public spaces. Consideration could be given to identifying–and strictly limiting and controlling–allowable sites for use by adults. This could serve to minimize normalization of marijuana and protect against the exposure of non-users to second-hand smoke and vapours. In addition, consideration will need to be given to the use of marijuana in workplaces. For example, a zero tolerance policy could be applied for those who operate heavy machinery or conveyances.
Questions
- How should governments approach designing laws that will reduce, eliminate and punish those who operate outside the boundaries of the new legal system for marijuana?
- What specific tools, training and guidelines will be most effective in supporting enforcement measures to protect public health and safety, particularly for impaired driving?
- Should consumption of marijuana be allowed in any publicly-accessible spaces outside the home? Under what conditions and circumstances?
5. Accessing Marijuana for Medical Purposes
Considerations
Courts have found that Canadians have a constitutional right to reasonable access to a legal source of supply of marijuana for medical purposes. A recent court decision found the MMPR failed to satisfy the constitutional requirement that there be “reasonable access” to marijuana for medical purposes.Footnote7
Determining how best to provide “reasonable access” to marijuana for medical purposes in the context of a legalized market for marijuana is not straightforward.
At a minimum, it seems clear that those whose medical needs cannot be met in a legal regime (e.g., those below the legal age or those who require a high-potency product if not legally available) will need a method of legal access.
Beyond that, it is the details of the legal regime created by governments (including production and distribution models) that will allow decision makers to determine whether a separate regime for medical users is required in order to provide “reasonable access” for medically-authorized marijuana users.
Limited experiences in other jurisdictions where separate medical and recreational markets coexist provide some interesting insights. For example, in Colorado, several stakeholders noted that the co-existence of retail and medical markets was problematic as it creates dual standards (e.g., different minimum ages, purchase quantities and taxation) and contributes to the grey market, therefore complicating regulation and enforcement. Some stakeholders have said that if they had the chance, they would have proceeded with recreational use only, instead of a dual recreational and medical system.Footnote8
In the 18 U.S. states that have medical marijuana regimes and where marijuana is not legal for recreational purposes, the production model varies between states:
- Seven allow commercial production and prohibit personal cultivation. A patient may only access medical marijuana from commercial producers that have been licensed by the government’s health department. Once a commercial cultivator is licensed, it must respect production limits, which are enforced in order to maintain public safety and to limit the diversion of marijuana to the black market.
- Three allow for personal cultivation only. In these states, the number of plants a patient may legally cultivate ranges from six to 15 mature plants at any given time. There are no provisions for commercial production and no licensed marijuana dispensaries. If a patient is unable to cultivate marijuana on their own, they are able to designate a grower to do so on their behalf.
- The remaining eight states allow individuals to choose personal cultivation or to purchase from state-licensed distributors.
Control of marijuana distribution in jurisdictions that allow for both personal and commercial cultivation can be a challenge. Marijuana produced commercially is tracked, which prevents producers from cultivating and holding material that is in excess of their plant limit. However, when personal cultivation is allowed, a grey market for products produced or distributed in ways that are unauthorized may be created.
In terms of quantities authorized for medical purposes, the range under the former Canadian personal cultivation regime is 0.5 grams/day to more than 300 grams/day, with average being 17.7 grams/day by December 2013. The College of Family Physicians of Canada suggests a maximum of 3 grams/day.
Possible Options
- Continued access to marijuana for medical purposes: It is anticipated that there could continue to be a need to enable access to marijuana for those who require it for medical reasons, but for whom reasonable access is not possible in the legalized context. This might require allowing different production methods (e.g., home cultivation) not available to others. It could also require carve-outs for medically-authorized youth or those who need high potency products. Physician involvement would still be necessary.
Questions
- What factors should the government consider in determining if appropriate access to medically authorized persons is provided once a system for legal access to marijuana is in place?
Conclusion
The subject of marijuana access and use is important, sensitive and complex, with issues and implications spanning health, public safety, and social and criminal justice policy domains. This discussion document presents key considerations for Canada’s approach to designing a system to legalize, regulate and restrict access to marijuana. It will be important to determine the most effective approaches to designing and implementing an effective system.
Addressing legalization requires input from all sectors and Canadians. In order to shape the best long-term approach for Canadians, engagement with experts, provinces and territories, and Canadians is key.
This document will be used to form the basis of discussions with provinces, territories and experts. All stakeholders – from governments and experts to Canadians – are invited to submit their views through the website.
Based on the comments received through engagement, the Task Force will draft a report that will be submitted to the Government to inform decisions on how best to legalize, regulate and restrict access to marijuana.
References
Bowes et al. (2013) Lifecourse SEP and tobacco and cannabis use European Journal of Public Health 23(2): 322-7.
Calvignioni et al. (2014) Neuronal substrates and functional consequences of prenatal cannabis exposure European Child and Adolescent Psychiatry 23(10): 931-41.
Canadian Centre on Substance Abuse. (2015) Cannabis Regulation: Experiences, Impacts and Lessons Learned In Colorado.
Centre for Addiction and Mental Health (CAMH). Cannabis Policy Framework. Toronto, ON: CAMH; 2014 Oct.
Chadwick et al. (2013) Cannabis use during adolescent development: susceptibility to psychiatric illness Frontiers in Psychiatry 4: 129.
Degenhardt and Hall (2012) Extent of illicit drug use and dependence, and their contribution to the global burden of disease The Lancet 379(9810): 55-70.
Degenhardt et al. (2013) The global epidemiology and contribution of cannabis use and dependence to the global burden of disease: results from the GBD 2010 study PLoS One 8(10): e76635.
Devinsky O, Cilio MR, Cross H, Fernandez-Ruiz J, French J, Hill J, et al. Cannabidiol: Pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders.
Epilepsia. 2014 Jun;55(6):791−802.
El Sohly et al. (2000) Potency trends of delta-9 THC and other cannabinoids in confiscated marijuana from 1980-1997. Journal of Forensic Science 45(1): 24-30.
EMCDDA Annual Report (2010) Risk Factors for Cannabis Initiation and Dependence http://www.emcdda.europa.eu/online/annual-report/2010/boxes/p45
Fergusson et al. (2008) Cannabis use and later life outcomes Addiction 103(6): 969-76.
George, T., & Vaccarino, F. (Eds.). (2015). Substance abuse in Canada: The Effects of Cannabis Use during Adolescence. Ottawa, ON: Canadian Centre on Substance Abuse.
Hall W, Degenhardt L. The adverse health effects of chronic cannabis use. Drug Test Anal. 2014 Jan−Feb;6(1−2):39−45.
Hall (2015) What has research over the past two decades revealed about the adverse health effects of recreational cannabis use? Addiction 110(1): 19-35.
Hartman RL, Brown TL, Milavetz G, Spurgin A, Pierce RS, Gorelick DA, et al. Cannabis effects on driving lateral control with and without alcohol. Drug Alcohol Depend. 2015 Sep 1;154:25−37.
Hartman RL, Brown TL, Milavetz G, Spurgin A, Gorelick DA, Gaffney G, et al. Controlled vaporized cannabis, with and without alcohol: Subjective effects and oral fluid-blood cannabinoid relationships. Drug Test Anal. 2015 Aug 10. doi: 10.1002/dta.1839.
Health Canada. Consumer Information–Cannabis (Marihuana, marijuana). Ottawa, ON: Health Canada; 2015 Dec. Available from: http://www.hc-sc.gc.ca/dhp-mps/alt_formats/pdf/marihuana/info/cons-eng.pdf
Health Canada. Information for Health Care Professionals–Cannabis (marihuana, marijuana) and the cannabinoids. Ottawa, ON: 2013 Feb. Available from: http://www.hc-sc.gc.ca/dhp-mps/alt_formats/pdf/marihuana/med/infoprof-eng.pdf
Heishman SJ, Arasteh K, Stitzer ML. Comparative effects of alcohol and marijuana on mood, memory, and performance. Pharmacol Biochem Behav. 1997 Sep;58(1):93−101.
Horwood et al. (2010) Cannabis use and educational achievement: findings from three Australasian cohort studies. Drug and Alcohol Dependence 110(3): 247-53.
Hussain SA, Zhou R, Jacobson C, Weng J, Cheng E, Lay J, et al. Perceived efficacy of cannabidiol-enriched cannabis extracts for treatment of pediatric epilepsy: A potential role for infantile spasms and Lennox-Gastaut syndrome. Epilepsy Behav. 2015 Jun;47:138−41.
Husni et al. (2014) Evaluation of Phytocannabinoids from High Potency Cannabis sativa using In Vitro Bioassays to Determine Structure-Activity Relationships for Cannabinoid Receptor 1 and Cannabinoid Receptor 2. Medicinal Chemistry Research 23(9): 4295-4300.
Leyton, M., & Stewart, S. (Eds.). (2014). Substance abuse in Canada: Childhood and adolescent pathways to substance use disorders.Ottawa, ON: Canadian Centre on Substance Abuse.
Loflin and Earlywine (2014) A new method of cannabis ingestion: the danger of dabs? Addictive behaviors 39(10): 1430-3.
Marihuana for Medical Purposes Regulations, SOR/2013-119. Available from: http://www.laws-lois.justice.gc.ca/eng/regulations/SOR-2013-119/
Meier et al. (2012) Persistent cannabis users show neuropsychological decline from childhood to midlife. Proceedings of the National Academy of Sciences 109(40): E2657-64.
Naftali T, Bar-Lev Schleider L, Dotan I, Lansky EP, Sklerovsky Benjaminov F, Konikoff FM. Cannabis induces a clinical response in patients with Crohn’s disease: A prospective placebo-controlled study. Clin Gastroenterol Hepatol. 2013 Oct;11(10):1276−80.
Porter BE, Jacobson C. Report of a parent survey of cannabidiol-enriched cannabis use in pediatric treatment-resistant epilepsy. Epilepsy Behav. 2013 Dec;29(3):574−7.
Public Health Agency of Canada. (2016) The Chief Public Health Officer’s Report on the State of Public Health in Canada, 2015: Alcohol Consumption in Canada.
Radhakrishnan et al. (2014) Gone to Pot–A review of the association between cannabis and psychosis Frontiers in Psychiatry 5: 54.
Rigucci et al (2015) Effect of high-potency cannabis on corpus callosum microstructure Psychological Medicine Nov 27: 1-14.
Rogosch et al. (2010) From child maltreatment to adolescent cannabis abuse and dependence: a developmental cascade model Development and Psychopathology 22(4): 883-97
Sewell RA, Poling J, Sofuoglu M. The effects of cannabis compared with alcohol on driving. Am J Addict. 2009;18(3):185−93.
Silins et al. (2014) Young adult sequelae of adolescent cannabis use: an integrative analysis The Lancet Psychiatry 1(4): 286-93.
UNICEF Office of Research (2013). ‘Child Well-being in Rich Countries: A comparative overview’, Innocenti Report Card 11, UNICEF Office ofResearch, Florence.
UNODC, World Drug Report 2012 (United Nations publication, Sales No. E.12.XI.1).
Vanyukov et al. (2012) Common liability to addiction and “gateway hypothesis”: theoretical, empirical and evolutionary perspective Drug and Alcohol Dependence 123 Suppl 1 S3-17.
Volkow ND, Baler RD, Compton WM, Weiss SRB. Adverse health effects of marijuana use. New Engl J Med. 2014 Jun 5;370(23):2219−27.
Annex 5: Executive Summary: Analysis of consultation input submitted to the Task Force on Cannabis Legalization and Regulation
Introduction
The Task Force on Cannabis Legalization and Regulation was given a mandate to engage with Canadians as the Government of Canada seeks to create a new system that will legalize, strictly regulate, and restrict access to cannabis.
Canadians responded to the Government’s Discussion Paper in unprecedented numbers, providing their suggestions and recommendations by means of an online consultation, as well as through other channels (email, letters, and detailed written submissions).
The feedback received – from Canadians, from provincial, territorial and municipal governments, and from experts, Indigenous governments and representative organizations as well as youth and those that use cannabis for medical purposes – will be instrumental in designing the appropriate system that fulfills the Government’s objectives.
Hill+Knowlton Strategies (H+K) conducted an analysis of the responses and submissions with the goal of informing the Task Force’s final report to government.
Our analysis is framed against the objectives of a new legalized cannabis regime as outlined by the Government of Canada and focuses on the five themes described in the Discussion Paper. Our team reviewed in depth the written submissions of the more than 300 organizations representing stakeholder groups that provided their views. In addition, the analysis included 28,800 responses to an online questionnaire organized under the five themes.
Each theme had its own questionnaire, requiring respondents to input their profiling information (age, region, gender) each time they provided input to a theme. Thus, a person who responded to all five themes, represents five total responses within the 28,880 total responses.
Almost all the online respondents identified as individuals, as opposed to organizations. Only 265 respondents identified themselves as representing an organization.
Online Questionnaire
Profile: Individuals
Consultation participants were asked to provide some basic socio-demographic information about themselves prior to proceeding to the questions. The exhibit below presents an aggregate profile of respondents.
Compared to the Canadian population as a whole, consultation participants were much more likely to be male, English-speaking, living outside of Quebec (particularly in Ontario, British Columbia (BC) and Alberta), younger (i.e., much more likely to be between 18 and 34 years of age), and possessing a higher level of formal education with a university degree or professional accreditation.
Figure 2 Profile: Individuals
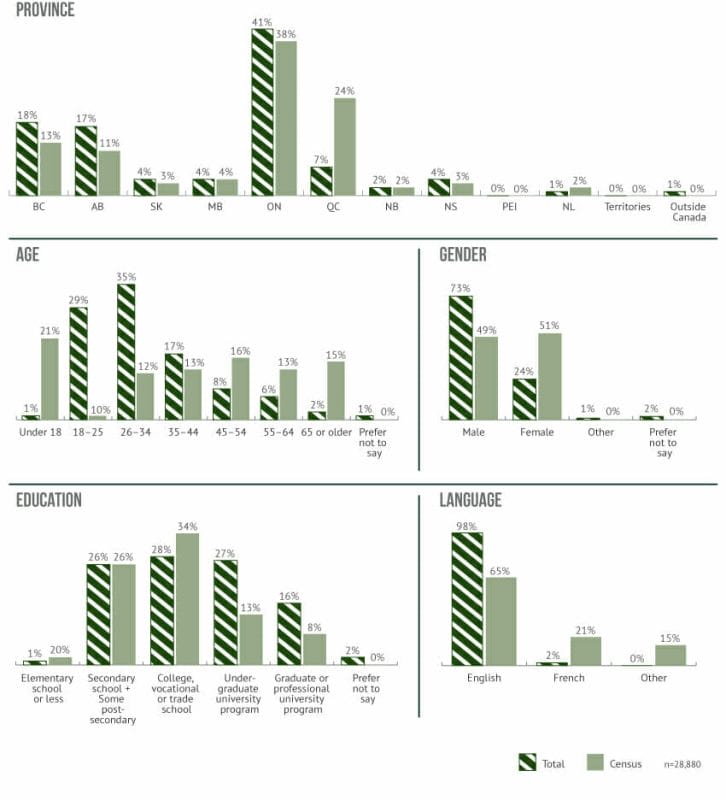
Figure 2 description
Other Key Characteristics
In addition to sociodemographic items, the consultation questionnaire included a question that asked individuals to describe themselves by choosing one or more descriptors from a broad list. As shown in the following list, close to half of the responses (49 per cent) came from individuals who describe themselves as users of marijuana for non-medical purposes. We also see a high level of participation from medical marijuana users (i.e., 30 per cent of responses).
Professions
11% The proportion of participants who are researchers or academics
8% The proportion of participants who are health-care professionals
Profile
15% The proportion of participants who are parents or guardians of a minor (under the age of 18)
Cannabis use
49% The proportion of participants that use cannabis for non-medical purposes
30% The proportion of participants that use cannabis for medical purposes
9% The proportion of participants that consider themselves cannabis activists
Profile: Organizations
In terms of the organizations who participated in the online consultation, they were more likely to describe themselves as NGOs/non-profits, followed by health-care associations/organizations. We also note that 13 per cent identified themselves as currently, or planning to, derive income from the production, distribution, or sale of cannabis.
Figure 3 Profile: Organizations
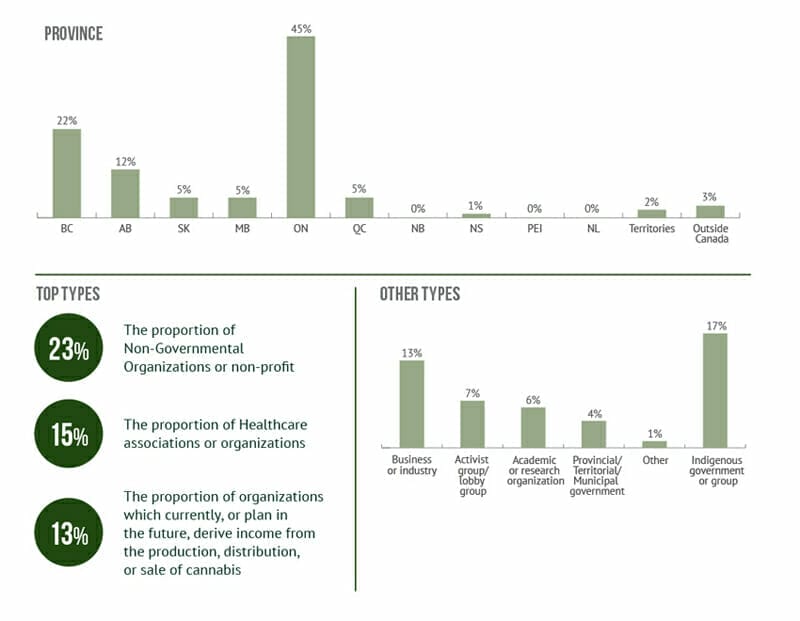
Figure 3 description
Submissions: Organizations
Type
Organizations 307
Sectors
Community Association 7
Government 27
Insurance 2
Law Association 7
Logistics/Supply Chain 20
Producer 36
Social Advocacy 44
Distributor 20
Health/Medicine 70
Labour/Workplace Safety 19
Law Enforcement 6
Patient Advocacy 38
Research 11
Types of submissions
Academic Paper
Author Manuscript
Bylaw
CV
Invitation
Letter
Policy paper
PowerPoint presentation
Report
Resolution
Standards Documentation
Article
Briefing Paper/Note
Committee Report
Invitation letter
Letter to the editor
Position paper
Radio PSA
Research Paper
White Paper
Channel
Emails to Cannabis email 186
Letters to Ministers and Prime Minister 91
Physical submissions 14
Online questionnaire 16
Thematic Focus
Theme 1: Minimizing Harms of Use 162
Theme 2: Establishing a safe and responsible production system 120
Theme 3: Designing an appropriate distribution system 151
Theme 4: Ensuring Public Safety and Protection 171
Theme 5: Accessing marijuana for medical purposes 129
Theme 1: Minimizing Harms of Use
This theme was the broadest in outlining the issues and options for designing the framework. It also garnered the most feedback overall in both the online and written submissions. The responses to the online survey and in the written submissions showed a strong level of support for some or all of the seven measures outlined in Theme 1.
Many of the online respondents provided additional recommendations aimed at minimizing harms and protecting children and youth. Support for the status quo was negligible, with many stakeholders expressing the need for a new “public health” approach to reduce the harms associated with cannabis use and improve the medical cannabis framework. There was a general recognition that the current regime puts an undue burden on individuals, the courts and law enforcement by criminalizing simple possession.
Responses to the online questionnaire indicated support for all or some of the measures outlined in the Discussion Paper, with many suggestions for refinement and improvement.
Figure 4: Measures for minimizing harms of use
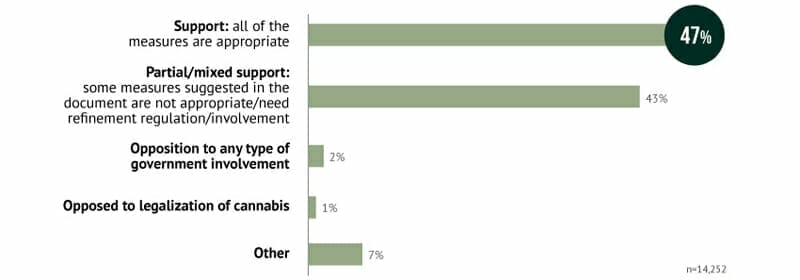
Figure 4 description
Minimum age for legal purchase
In the online questionnaire, suggestions varied from no age limits to prohibiting use by those under 25 years of age. The clear majority, however, suggested that the age limit should be set at somewhere between 18 and 21 years of age.
Many public health organizations and medical professionals pointed to the scientific evidence that the human brain does not fully develop until 25 years of age, which puts children and youth at increased risk of harm. However, many of these organizations acknowledged that setting a minimum age at this level will likely drive users into the illicit market, continue to criminalize cannabis possession, and burden the courts.
Most respondents wrote that the age restriction for cannabis should be the “same as alcohol.” “Consistency,” “simplicity” and “harmonization” were watch words among those who advocated setting the minimum age at the same level as alcohol.
Figure 5: Minimum age for legal purchase
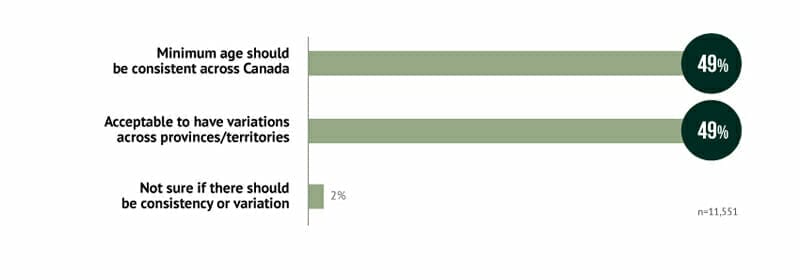
Figure 5 description
A range of public health and other experts recommended that the federal government should set the minimum age and that the provinces and territories should be able to raise the age but not lower it.
“If a federally set age limit can be set, if possible legislatively, it would be a strong precedent for standardization across Canada.”
– College of Family Physicians of Canada
Advertising and marketing restrictions to minimize the profile and attractiveness of products
Most online respondents were supportive of measures proposed in the Discussion Paper, including measures that would strictly limit marketing, advertising and promotion of cannabis products.
Some individuals and industry representatives expressed the view that advertising and marketing should be permitted to differentiate between products and potencies, and advised against the wholesale adoption of Canada’s tobacco model. The most prevalent argument was that emulating Canada’s approach to tobacco was inconsistent with their view that “cannabis is objectively less dangerous than both alcohol and tobacco.” Many of these respondents believed the regime should adopt the same approach as alcohol in the marketing and promotion of cannabis products.
However, public health experts, law enforcement, and municipal government representatives indicated strong support for strict controls on product promotions, with participants often linking these to the protection of children and youth.
As one respondent indicated:
“We recommend that any advertising, promotion, and sponsorship of legal cannabis products be prohibited.”
Many experts expressed agreement with the Cannabis Policy Framework developed in 2014 by the Centre for Addiction and Mental Health (CAMH), which said:
“There should be a total ban on marketing, promotion, and advertising, and products should be sold in plain packaging with clear product information and warnings about health risks.”
Organizations representing Canada’s physicians and nurses also recommended restrictions on marketing and promotion of tobacco products. Public health organizations often referred to measures that have been successful in reducing smoking rates in Canada to among the lowest in the world. These are seen by many as crucial to ensuring that youth do not come to view the use of cannabis as normalized adult behaviour.
Taxation and pricing
Taxation and pricing policies are viewed as an important tool in reaching the Government’s objective of minimizing harms associated with cannabis use. These revenues can support the efforts of governments and health agencies to educate Canadians and offset additional costs such as substance abuse treatment, licensing and enforcement.
Many online comments pointed to the need for government to develop a taxation and pricing regime that strikes a balance between generating tax revenue and curbing demand for illicit market product. In this vein, many individuals and experts also pointed to tobacco taxation policies in Canada as a solid model upon which to base the cannabis taxation and pricing regime. Limiting the demand for illicit market product was viewed as important for keeping cannabis out of the hands of underage youth.
There was also strong agreement among stakeholders in law enforcement and health, and among local governments that cannabis taxation revenues should be shared by all levels of government to address health and social problems related to drug use. Revenues can be directed away from criminal enterprises towards harm reduction, public awareness, appropriate enforcement, treatment programs and research.
The Canadian Public Health Association, for example, recommended that:
“All tax revenues from the sale of cannabis and related products be directed back to support the establishment and management of the programs and activities necessary to manage its legalization and regulation.”
Restrictions on cannabis products (THC)
According to the Discussion Paper, the potency levels for THC, the psychoactive ingredient in cannabis, have increased dramatically in the past few decades, and this trend is likely to continue because of technology and innovation.
Experts pointed to a lack of research on how these high-potency strains of cannabis specifically impact the human brain, especially youth, in arguing for strict limits on THC levels. However, there was agreement among health experts that higher concentrations have the obvious potential to cause more harm, especially to youth, and will have an impact on road and workplace safety.
The Canadian Centre on Substance Abuse advocated for a precautionary approach in regulating potency levels:
“If the primary objective is public health, restrictions should be implemented, at least initially, to allow time for research on the health impacts of high-THC products. If the primary objective is reducing the influence of the illegal market, higher-potency products should be permitted, but subject to escalating minimum price levels.”
The Canadian Public Health Association argued for strict limits on THC levels:
“A THC concentration of 15% should be established as the maximum permitted for usable cannabis products (including the dry product, creams, salves and oils) sold under this legislation and these regulations. Oils and other products having higher THC concentrations (greater than 15%), which are used for therapeutic purposes, should not be sold for recreational use.”
However, some of the online comments expressed concerns about limiting potency levels for several reasons, citing individual freedom, concerns about the illicit market and increased health risks because users will smoke or ingest more cannabis to get the desired effect.
Figure 6: Restrictions (potency, advertising, taxation, etc.)
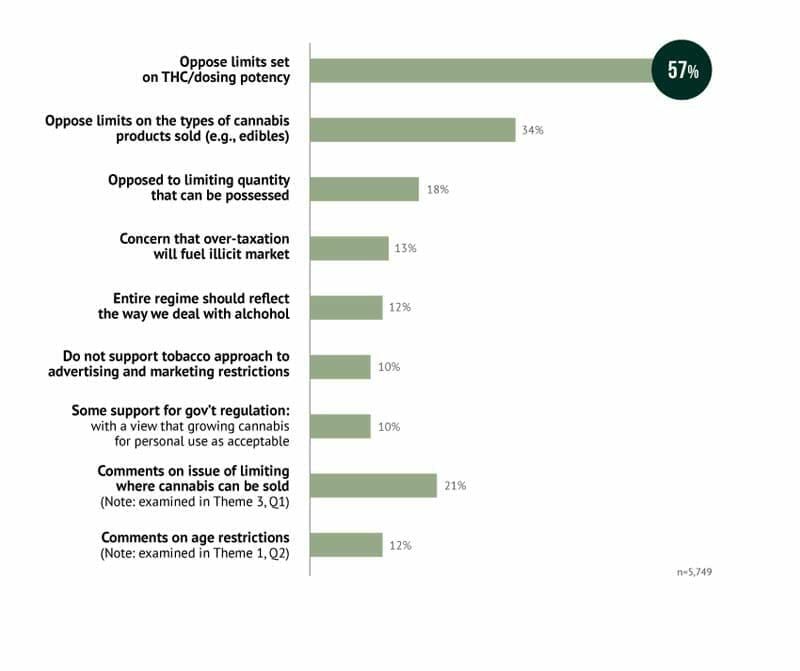
Figure 6 description
Restrictions on cannabis products (types)
There is a growing list of cannabis-based products like foods that could be especially harmful to children if consumed accidentally and respondents expressed concerns that products such as candies could be designed to appeal to youth with obvious negative consequences for public health.
However, other respondents felt that imposing restrictions on edibles would have the unintended effect of leading users to smoke the product to achieve their desired high and thus increase risks to their health. It was also seen as unnecessarily inconveniencing those who cannot or do not want to inhale smoke, or prefer the type of low dosage contained in some edibles.
The other key argument against placing restrictions on cannabis products such as edibles was a desire to see consistency between Canada’s cannabis policies and the way in which governments regulate other products that can cause harm to children such as alcohol, over-the-counter medication, household cleaning products, matches and lighters. Respondents pointed out that clear labelling, secure and well-designed child proof packaging, and encouraging parental responsibility can protect children from harm.
Some public health and health professional organizations called for scrutiny of any products that could target youth and children. There were also concerns expressed about children unknowingly ingesting foods or candies containing cannabis.
“Some of the highest-potency products, e.g. some cannabis concentrates and synthetic cannabinoids, may have to be banned altogether. Products designed to appeal to youth via flavour or appearance should be prohibited as well.”
– Centre for Addiction and Mental Health
Limitations on quantities for personal possession
When considering whether there should be limits on personal possession, many stakeholders believe there ought to be a balance. In examining other jurisdictions, limits have been imposed on personal possession. However, some organizations and individuals point out that there are no such limits for possession of restricted products like alcohol or tobacco.
In the online consultations, 18 per cent expressed concerns about placing limits on quantities for personal use. As one respondent put it:
“There should be no limitation on quantities possessed for personal use; some people collect wine or cigars, why should marijuana be any different?”
These concerns were also shared by the Canadian Bar Association:
“We question whether any limits make sense in a legal market, as people are not currently limited in the amount of alcohol or tobacco they can legally possess.”
However, many organizations, from municipalities to public health and others, argued that it is reasonable to place a limit on the amount of cannabis that can be possessed by an individual. Many proposed that a policy decision should reflect the public health approach which minimizes the harm associated with criminalization, discourages diversion to the illicit market and protects children and youth.
“Imposing reasonable limits on quantities for possession – for example, 28 grams for consistency with those imposed in legalized states in the U.S. – is a reasonable precautionary step to help establish lower-risk patterns of use as social norms develop under a legal regulatory framework.”
– Canadian Centre for Substance Abuse
Limitations on where cannabis can be sold
Distribution is further explored in Theme 3, but respondents were also invited to weigh in under Theme 1. As shown below, many comments described a preference for a mixed public-private system, which blends direct government involvement with private licensed retailing through storefronts such as pharmacies and dispensaries.
Figure 7: Where cannabis can be sold
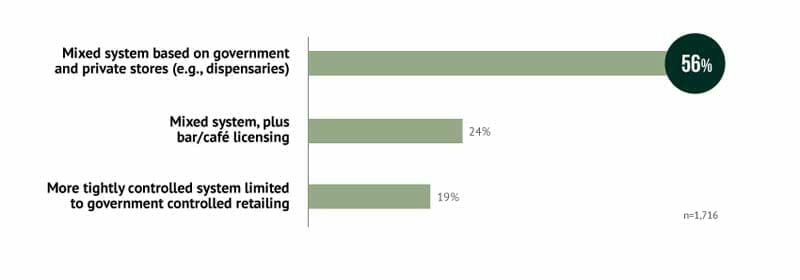
Figure 7 description
Our analysis of the online responses reveals that opinions on this important question can be categorized into three groups, along a continuum of ease of access.
- Tight control, limited to direct government involvement in retailing (i.e., the way that liquor is retailed in some provinces, such as the LCBO in Ontario);
- Mixed public-private system with private retailing limited to pharmacies and dispensaries; and
- Mixed public-private system, but with the addition of licensed sales in bars, cafés and restaurants, along the lines of liquor licenses.
Some online respondents felt that selling cannabis in dispensaries would allow purchasers to benefit from expert advice. While this approach has benefits for consumers, it is also seen as something that could help to reduce harms by offering users advice on issues such as dosage and potency.
Many online respondents were uncomfortable with the idea of a “government monopoly” over cannabis – some for philosophical reasons, but most out of practical concerns, such as not wanting to encourage illicit market consumption by unduly limiting access.
On the other hand, some public health agencies recommended a government-controlled regime as the best model for reducing potential harms, especially for children and youth.
Municipalities have noted that they will be directly impacted by the presence of cannabis outlets, whether they are storefront outlets or dispensaries of cannabis for medical purposes.
Theme 2: Establishing a Safe and Responsible Production System
Five questions were posed under this theme, with Canadians providing input on the establishment of a safe and responsible production system.
Production model
The graph below shows many Canadians who responded online favour an approach that allows for a mix of home cultivation and licensed cannabis producers.
Figure 8: Production models
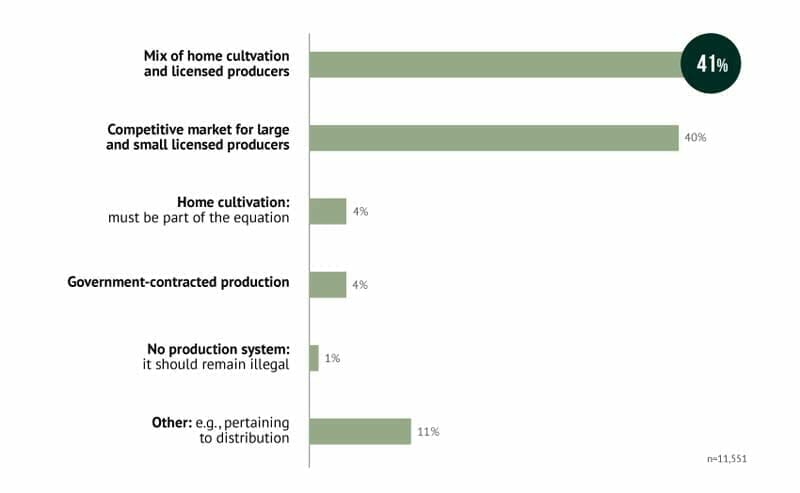
Figure 8 description
A production system based on licensed producers but that also allows home cultivation for personal consumption was described in 4 of 10 responses as the preferred production model. Concerns were often expressed about the need to balance regulation (e.g., to ensure quality) with competition, to ensure variety and competitive pricing.
Quite a few responses suggested that a mixed model based on home cultivation and government-regulated commercial production should mirror what is currently in place for beer and wine – allowing homemade production with minimal regulation, as well as large-scale commercial production and small craft production, with greater regulation.
This is an issue where there was a divergence between the online responses from Canadians and the perspective of many public health organizations that believe a government monopoly is the best approach to control and regulate production and distribution of cannabis.
A common response from these experts was that, based on the experiences of other jurisdictions that have legalized cannabis, it is much easier to take a more restrictive approach at the outset and loosen the regulations later than try to tighten the rules after the regime is in place in the event of unforeseen consequences.
Local governments pointed out that they will be on the “front lines” in the regulation of producers and that there will be a direct impact on health and safety in their communities. Many advocated for a regime that allows for strict oversight and regulation and close co-operation between federal, provincial, territorial and municipal governments in establishing the production regime.
“Municipal governments must be able to license marijuana producers and distributors. This helps municipal governments control the location, the concentration and siting of marijuana businesses as well as the ability to respond to community concerns.”
– Association of Municipalities of Ontario
Municipal governments also advocated that revenues derived from a licensing regime should be used to offset increased costs for oversight and enforcement of standards.
Home cultivation
There was a clear consensus among respondents to the online survey that home cultivation should be allowed as part of the new regime.
As one respondent to the online consultation put it:
“Private production and home cultivation would be most appropriate and allow consumer demands to be met.”
Figure 9: Home cultivation
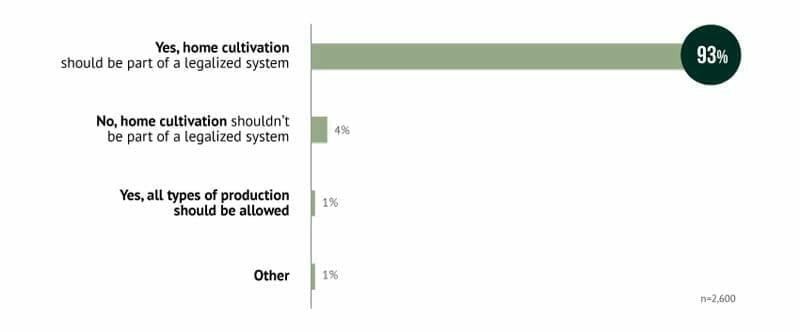
Figure 9 description
However, some public health groups warned that home cultivation will increase the risk of cannabis products falling into the hands of children and youth and make it difficult to determine potency levels. Municipalities were concerned about the increase in grow operations that could pose a risk of fire, mould and other health and safety hazards.
Some recommended a cautionary approach to home cultivation:
“Home cultivation should likely only be permitted for personal use when medical access to marijuana is required. Retail sale should likely not be permitted with home cultivation. Strict federal regulations will need to be implemented on the number of plants permitted per person and per household to ensure that large grow operations do not become prevalent.”
However, there was a recognition that banning home cultivation altogether would lead to increased criminalization of individuals and growth of the illicit market. Submissions pointed to the United States (U.S.) where Alaska and Colorado allow for modest levels of cultivation for personal use. Some have argued that home growers should be required to pay a modest licensing fee.
“Banning home growing for personal use defeats the purpose of legalization, which is to reduce the harms of criminalization.”
– College of Family Physicians of Canada
Licensing and fees
As indicated below, a strong majority of online responses expressed support for some form of commercial production licensing to maintain quality standards and to reduce illegal production and sales.
Figure 10: Licensing and fees
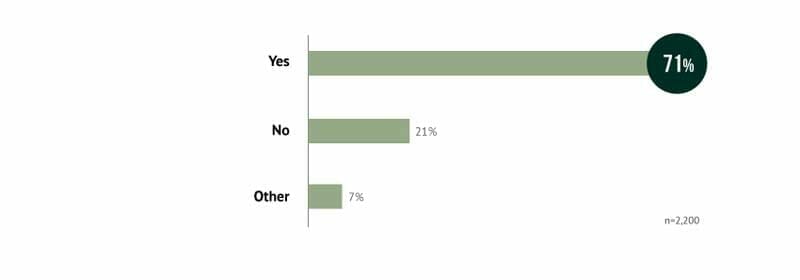
Figure 10 description
Some respondents urged that the cost of licences and other fees be affordable to allow smaller producers into the market and to help foster healthy competition.
Others commented that licensing fees should cover the cost of maintaining proper inspections and regulations within the production system. This recommendation was widely supported by local governments and health agencies. Many of these organizations also believe that revenues from licensing could also be directed towards law enforcement, treatment programs and other activities aimed at reducing harm. Municipalities believe that licensing is a key tool in protecting the health and safety of their communities.
Requirements for production, packaging, storage and distribution
There was widespread agreement among stakeholders and experts that strict controls are necessary to assure product quality, security and safety, and to minimize diversion to the illicit market. The Canadian Nurses Association and others recommended that a new regulatory framework should contain features designed to ensure good manufacturing practices.
The Cannabis Trade Alliance of Canada, which represents producers, said the new regime should provide for mandatory testing:
“Mandatory laboratory testing of all cannabis products (potency and contaminants) – a critical step in the seed-to-sale process when considering public health, and should be the main objective in the legalized framework.”
According to the Alliance, this would encourage best practices in all phases of production, including licensing, testing, tracking, inventory control, as well as health and safety. There was a consensus in the submissions of experts and stakeholders that product packaging and labeling must be strictly regulated in the interests of public health and safety.
Role of Existing Producers Under the ACMPR
Many of the respondents to the online survey believed that existing producers should be allowed to participate in the new regime.
Suggestions from some expert stakeholders called for strengthening of the requirements as set out in the Access to Cannabis for Medical Purposes Regulations(ACMPR) to develop a more comprehensive regulatory system that would include the development of national standards for production, packaging, storage, distribution and testing of cannabis products. The system would regulate a wider variety of cannabis products such as edibles, concentrates and tinctures. The appropriate resources would be necessary to inspect and enforce the regime.
Some concerns were expressed in the online consultations and in the submissions by patient organizations about the limitations of the current medical cannabis regime and the affordability of products. They saw this as an opportunity to fix some of the problems that have been identified.
Some online participants recommended development of standards to govern the use of pesticides, labelling standards, regulations around the “organic” designation, employee health and safety, security of production facilities, and basic product quality and safety standards.
Theme 3: Designing an Appropriate Distribution System
The distribution model
As indicated below, a strong majority of online comments suggested that the best distribution model would consist of privately-owned storefronts or dispensaries, acted upon by market forces. This option was most popular among those that use cannabis for medical and non-medical purposes and self-described activists.
The advantage of the storefront model, according to many online respondents, would be to foster competition that would keep prices low and discourage the illegal market.
Some online respondents expressed dissatisfaction with the current mail-order option for cannabis for medical purposes and saw it as justification for moving to a private storefront model. It should be noted, however, that even those who complained about the problems of mail-order cannabis only very rarely called for abolishing it.
Several organizations recommended that staff who work in storefront operations should receive special training and that measures should be taken to ensure the health and safety of children and youth. The Canadian Association of Chiefs of Police (CACP) received feedback from its members expressing concerns that organized crime might try to get involved in storefront operations and that measures should be taken to keep this from happening.
Variation across provinces and territories
In the online survey, local choice was the second-most-popular model, although it was contained in only 10 per cent of comments to this question. For the most part, “local choice” was understood as leaving decisions on appropriate distribution mechanisms to the provincial and territorial governments.
Those who supported local choice believed the provinces and territories are best placed to decide which distribution model would be most suitable for their communities. Different jurisdictions, and especially urban and rural areas, have different challenges which should be reflected in cannabis distribution.
Many of the organizations that commented on this issue urged the federal government to take a leadership role in establishing the distribution model in collaboration with provincial, territorial and local governments.
The Federation of Canadian Municipalities recommended that all retailers that distribute cannabis be licensed similar to producers. This would help to identify which retailers are operating with permission from local authorities and guard against opening in locations frequented by youth and children. Licensing could also ensure that the design of storefronts does not glamorize the use of cannabis. Denver was cited as an example of where this approach has been implemented.
When it comes to storefront operations, it was widely perceived by public health organizations and experts that alcohol and cannabis should not be available on the same premises. Several submissions and online comments pointed to the potential economic benefits of the new regime which would create jobs and revitalize communities.
Other models worthy of consideration
There was limited support for a government-controlled system among online respondents. Analysis suggests that the primary concern was that cannabis distribution in Canada should not be the exclusive purview of government-owned stores. Many consultation participants in the online questionnaire offered the opinion that Canada’s cannabis production and distribution systems should be shaped by market forces because competition is the best way to foster a regime with a wide range of high-quality products at affordable prices and to encourage innovation. Simply put, the more competition there is, the better it will be for the consumer.
However, a government model based on the LCBO or SAQ was favoured by some public health, municipal and health-care professional organizations. Many of the stakeholders and experts urged the Task Force to draw upon lessons learned from U.S. jurisdictions where cannabis has been legalized.
This point was reinforced by the Ontario Public Health Unit Collaboration on Cannabis, which says that:
“Government ownership is the most effective way to achieve the overall government goals of reducing harm related to marijuana consumption.”
However, the Cannabis Trade Alliance of Canada said businesses should have the opportunity to participate in the new regime, adding that:
“Provincial regulations should allow for the issuing of cannabis distribution and sales licenses to businesses that are compliant with all applicable rules and regulations.”
Theme 4: Enforcing Public Safety and Protection
Designing the appropriate laws
Designing laws that discourage illegal activity is another delicate balancing act, given the objectives of improving public health and minimizing harm while also reducing the burden on law enforcement and the justice system.
The online responses often described a regime modelled on current alcohol regulations. This is based on the belief that the legal and regulatory framework around alcohol has been successful at discouraging minors from accessing alcohol through retail stores, bars and restaurants. Some respondents pointed out that the heavy fines and other sanctions that are in place for infractions such as selling to minors seem to be providing effective deterrence.
Figure 11: Designing the appropriate laws
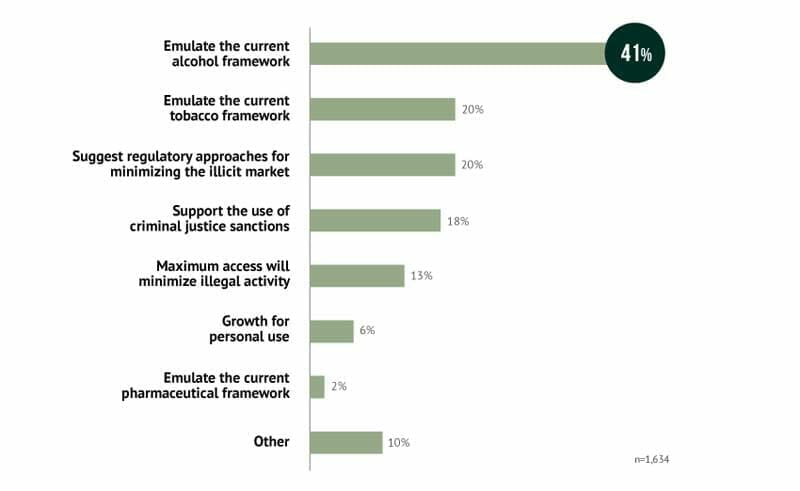
Figure 11 description
There was also appeal in the way in which current legislation allows police and the courts to deal with those who drive while impaired by alcohol, including potential jail time for the drivers if others are injured or killed.
Some respondents suggested that the best way to reduce the number of Canadians operating outside the regime is to allow access to cannabis with little or no regulation.
Those who wrote about the use of criminal justice sanctions often linked this to one of three spheres of activity: 1) organized crime; 2) impaired driving; and 3) distribution to minors. If anything, these respondents were more likely to call for a stiffening of the penalties that are currently in place, with some adding that police, prosecutors and the courts will be in a better position to identify and deal with serious offenders once cannabis becomes legal.
As one respondent put it:
“Enforcement efforts should be aimed at stamping out organized criminal activity, large-scale black market production, distribution, and trafficking.”
The Canadian Association of Chiefs of Police received feedback from its members which raised concerns that organized crime will attempt to infiltrate a recreational cannabis regime. Some members who responded to the CACP survey noted that organized crime is already benefitting from the former Marijuana Medical Access Program, and said there was evidence that organized crime already owns and operates licensed grow operations. In addition, the input from members also included concerns that criminals will continue to exploit the illicit market to maintain their illicit enterprises.
“Organized crime could be expected to produce high potency strains of dried marijuana products that are not permitted under the new legalized regime. These products may be more attractive to users and then sold illegally. These products would be produced to entice marijuana consumers to the black market.”
– Canadian Association of Chiefs of Police
The Canadian Bar Association recommended that cannabis be removed from the Controlled Drugs and Substances Act (CDSA) so that cannabis use, production and distribution can be regulated across Canada in a manner like other non-criminal, regulated substances.
“Setting up a system where marijuana is partly regulated by a new regulatory regime and partly criminalized under the CDSA would be confusing and challenging. It again raises questions as to which level of government would regulate, and who should enforce and prosecute those regulations. In a legal market, the need for any offenses is questionable, especially as marijuana is not addictive in the scientific meaning of that word.”
– Canadian Bar Association
The community of Duncan, BC, submitted that the lion’s share of the work for regulation and enforcement of retail dispensaries may well fall to local governments. Duncan’s City Council asked that a portion of any future federal or provincial taxes collected through cannabis sales and distribution be shared with local governments, perhaps like the Federal Gas Tax program. This would provide more resources to hire and train staff to ensure appropriate enforcement.
Tools, training and guidelines to protect public safety including impaired driving
A significant number of consultation participants, whether online or in written submissions, expressed the view that awareness, information and education will be key to success, particularly where youth and parents are concerned.
As shown below, many comments (40 per cent) referred to the need to conduct research into the effects of cannabis on drivers and to develop best practices for deterring and reducing impaired driving. About one in three comments stressed the importance of investing in new tools for the detection of drug-impaired driving.
Analysis of the comments pertaining to the development of new tools revealed the presence of two widely held points of view: 1) driving while under the influence of cannabis poses a threat to public safety; and 2) current technology and approaches for detecting cannabis are very likely inadequate.
Figure 12: Tools, training and guidelines to protect public safety including impaired driving
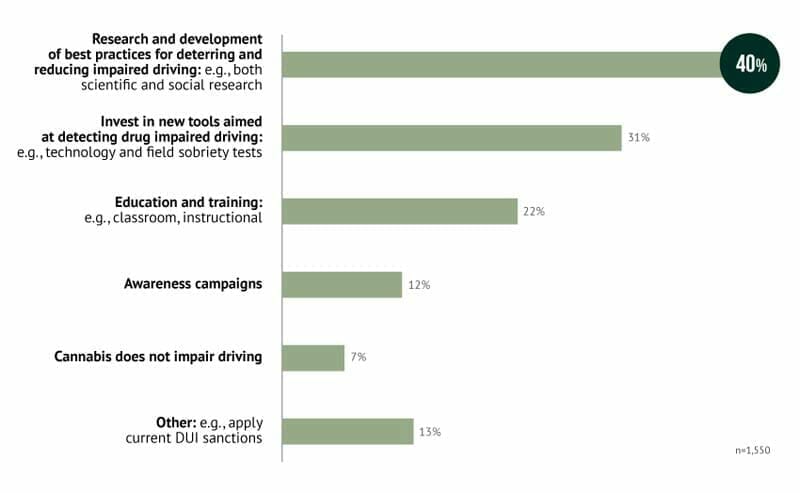
Figure 12 description
These comments were echoed in the submissions of many expert stakeholders who said measures need to be in place for detection, enforcement and prevention of cannabis-impaired driving.
Organizations like Mothers Against Drunk Driving (MADD) have recommended that the federal government amend the Criminal Code to create a per se impaired driving offence for having care and control of a motor vehicle with a THC level above a prescribed limit. MADD believed that limit should be set at a level akin to the .05% Blood Alcohol Content (BAC) limit for drinking and driving and recommended that the federal government enact a system of mandatory roadside saliva testing for cannabis and other commonly-used drugs, adapting the model of Europe and Australia.
Additional challenges identified by the police chiefs include; a lack of skills and a shortage of trained officers to determine impairment from cannabis or other drugs, there is no approved method of testing and detection at the roadside, the time consuming process to obtain a blood sample from a suspected impaired driver and a lack of data and research on “appropriate levels.” Further, there is no quantitative measurement of impairment in the Criminal Code or a provincial statute, as there is with alcohol.
Due to the way THC is absorbed in the body and the current challenges with identifying drug impaired drivers, the CACP supports a zero tolerance enforcement approach with driver’s who utilize drugs, including cannabis, and chose to drive while their ability to do so is impaired. Once evidence based data is available an informed decision can be made regarding the appropriate per se limit that will further assist officers in determining indicia of impairment in a driver.
Many online respondents expressed the opinion that levels of impairment after ingesting cannabis can differ based on the individual.
As an example, one commented:
“An arbitrary legal blood level, as used in Washington State, does not accurately reflect impairment, particularly in regular users.”
Stakeholders pointed to the fact that, currently, there are fewer than 600 officers trained in drug evaluation and classification. Many organizations pointed to the need to expand officer training across the country and some recommended that toxicological laboratories should have additional capacity to analyze blood samples for drugs in a timely manner.
The Canadian Automobile Association (CAA) cited recent U.S. studies from Colorado and Washington which point to an increase in cannabis-related traffic fatalities following legalization, as well as concerns about higher levels of impairment when both drugs and alcohol are involved. However, there has been limited research in this area.
Many organizations, experts and online contributors wanted to see improved support from government for research and data collection activities so that evidence-based decisions can be made post-legalization on any required enhancements to the law.
Along with detection and enforcement provisions, there was strong support for ongoing public education campaigns aimed at informing Canadians – and especially our youth – on the harms associated with drug-impaired driving.
One contributor to the online consultation put it this way:
“Training should be offered in schools to reduce the risks of impaired driving as well as television campaigns and the Web to reach the largest audience.”
Organizations representing employers recommended that more attention needs to be placed on the impact that a new regime would have on the workplace, especially for those employees who work in sensitive positions where impairment can put public health and safety at risk.
For example, FETCO, the association representing federally regulated employers in transportation and communications, called on governments to develop regulations prohibiting all employees in safety-sensitive positions in federally regulated industries from consuming cannabis in the workplace or being under the influence of cannabis at any time while on or preparing for duty. Governments and key stakeholders should work collaboratively to examine how labour and human rights legislation might be impacted by issues surrounding cannabis and the workplace including the use of cannabis for medical purposes.
Restricting consumption to the home or a limited number of well-regulated publicly accessible sites
Half of the online survey comments suggested that cannabis should be treated the same as tobacco, a view that was more prevalent in comments made by those under 45 years of age. Here, it is reasonable to assume that these respondents were thinking of people using cannabis by smoking it. As seen throughout this report, there is a common-sense appeal to drawing heavily on current “tried and tested” alcohol and tobacco controls for the development of a policy framework for cannabis.
Consultation participants had different views about where cannabis could be legally consumed depending on the method of ingestion (e.g., smoking, vaping, eating). About one-third of respondents believed that it would be acceptable for cannabis that is not smoked to be consumed in establishments that are licensed to sell the product.
One online respondent put it this way:
“There should be safe places for adults to consume the substance where underage persons are not allowed. Those places should follow the model of Netherlands cannabis cafes. Also, those places should not allow alcohol consumption.”
Many drew parallels to alcohol regulations which allow for consumption in licensed establishments and designated outdoor areas. Some cited the importance of ensuring that cannabis-licensed establishments should be a minimum distance from schools and possibly other places where children congregate.
There was also a significant number of consultation participants, especially among those that use cannabis for medical purposes, who indicated support for a legal framework that would allow people to smoke cannabis in private clubs, with “proper ventilation.”
At the municipal level, some communities have recommended that enforcement of public consumption should be consistent nationally.
As one respondent recommended:
“Establishing a regulatory model for cannabis should ensure use is prohibited in places where tobacco smoking or e-cigarette use is also prohibited. This will ensure consistency with existing laws and address potential health concerns associated with second-hand cannabis smoke and vapour, and social exposure of youth to smoking.”
Theme 5: Accessing Cannabis for Medical Purposes
Overall, Canadians and stakeholders recommended that the regime should be designed in a way that suits the needs of all Canadians who require cannabis for medical purposes while maintaining effective controls to reduce potential harms.
Accessibility for medical purposes was largely viewed by respondents across three dimensions: affordability, availability and effectiveness.
About one-third of respondents felt that allowing home cultivation is the best way to ensure access for users of cannabis for medical purposes. Cost was identified as a barrier, followed very closely by the impact that various distribution models could have on access. About one-fifth of comments pertained to the availability of product (e.g., ensuring continued availability of strains and potencies).
Fewer comments were made concerning the role of physicians and relatively few comments (six per cent) specifically addressed the merits of having separate systems of cannabis for medical and non-medical purposes.
For many of the medical cannabis users who responded to the survey, the issues of home cultivation and affordability are linked.
As one respondent put it:
“Without my ability to grow my medicine myself I would not be able to maintain my present state of health.”
The concerns raised by respondents online were echoed by patient organizations that are calling for broader access and measures aimed at affordability, such as sales tax exemptions. In a joint submission, the Arthritis Society, Canadians for Fair Access to Medical Marijuana and the Canadian AIDS Society urged the government to approve a wide range of distribution options, including on-site dispensing, mail-order and self-production.
Organizations representing pharmacy and the supply chain recommended that pharmacists be authorized to dispense cannabis for medical purposes to an individual with a medical document. They contended this would allow for better tracking and consistency of product with a secure and traceable supply chain and would enhance patient safety.
Although few online participants commented on whether there should be separate regimes for the use of cannabis for medical and non-medical purposes, several stakeholders – including the Canadian Medical Association and the Canadian Centre on Substance Abuse – recommended that the two should be integrated as much as possible to achieve efficiency and reduce diversion. Allowances could be made to accommodate youth and those who require more potent products when supported by a medical professional.
“The Canadian Medical Association recommends that there be only one regime for marijuana, following legalization of non-medical marijuana, with provisions for the medical needs of those who would not be able to acquire marijuana in a legal manner, e.g., those below the minimum age or those with a requirement for a more potent product than legally available.”
– Canadian Medical Association
The feedback almost unanimously called for more research on cannabis for medical purposes to assess potential benefits and risks in the short and long term and for development of appropriate treatment regimes. Some public health organizations called for a portion of tax revenues to be directed toward research.
“Since so far, no scientific studies have shown that marijuana encompasses benefits that can relieve the symptoms of certain diseases, ASPQ recommends that part of the tax collected from the sale of marijuana products be allocated to research to allow further investigation on the topic.”
– L’Association pour la santé publique du Québec
Observations
The public consultations on the design of a new legislative and regulatory system for restricted access to cannabis elicited feedback from nearly 1,500 individuals and organizations as well as 28,800 online responses. The responses and recommendations from Canadians, experts and organizations representing public health, governments, health-care professionals, patient organizations, industry and others were wide-ranging and informative. In summarizing that feedback, there is ample evidence that Canadians support a new regime that meets the nine objectives as outlined by the Government of Canada, and many individuals and organizations offered valuable recommendations for refinement and improvement.
- A public health approach is the right approach in designing a new regime. All levels of government need to collaborate to ensure the system meets the objectives set out in the Discussion Paper.
- Education and public awareness are fundamental to the successful implementation of the new regime; programs should be in place prior to its launch.
- Portions of revenues from the taxation of cannabis should be directed towards education, research, treatment, enforcement and other initiatives that minimize harm and protect children and youth.
- Impaired driving and workplace health and safety are issues that need urgent attention as the new regime is developed.
- There are significant gaps in the knowledge and understanding of the impacts of cannabis use for medical and other purposes; more support for research is needed.
Footnotes
- Footnote 1
- The CDSA is the Act that regulates activities with controlled substances (prohibiting possession, trafficking, possession for the purposes of trafficking, importing, exporting, possession for the purposes of exporting, and production) and sets out the associated criminal offences and penalties for violating these prohibitions. The CDSA is also the law that fulfills Canada’s international drug treaty obligations.
- Footnote 2
- Production includes both the cultivation and the manufacturing, or processing, of cannabis.
- Footnote 3
- Delivered on April 20, 2016. http://news.gc.ca/web/article-en.do?nid=1054489
- Footnote 4
- Used here with permission from the authors. Rolles, S. & Murkin, G. (2016) How To Regulate Cannabis: A Practical Guide. 2nd ed. Transform Drug Policy Foundation. Available from: http://www.tdpf.org.uk/resources/publications/how-regulate-cannabis-practical-guide. [Marks, J. The Paradox of Prohibition in “Controlled Availability: Wisdom or Disaster?”; National Drug and Alcohol Research Centre, University of New South Wales; p. 7-10. 1990.]
- Footnote 5
- http://www.lcbo.com/content/lcbo/en/corporate-pages/about/media-centre/quick-facts.html#.WC385LIwiUk
- Footnote 6
- From the Chief Medical Officers of Health report, Public Health Perspectives on Cannabis Policy and Regulation
- Footnote 7
- Allard et al v. Canada: Federal Court. February 24, 2016.
- Footnote 8
- Canadian Centre on Substance Abuse. Cannabis Regulation: Experiences, Impacts and Lessons Learned In Colorado. June 2015.