
Phase 3
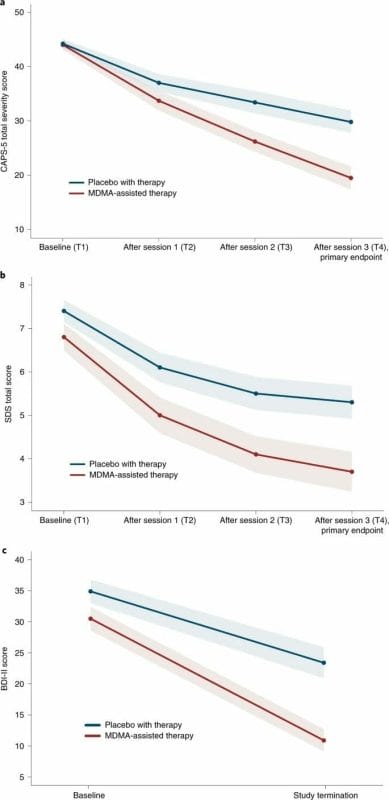
Today MAPS released the results of its highly anticipated phase 3 MDMA assisted therapy for severe PTSD study. The results are what many, including myself, anticipated – significant.
Fifteen study sites were used, 11 in the United States, two in Canada, and two in Israel. Participants were randomized in a blinded fashion and were allocated 1:1 to either the MDMA-assisted therapy group or the placebo with-therapy group. Those taking the MDMA and placebo were given three doses.
According to MAPS,
Compared with current first-line pharmacological and behavioral therapies, MDMA-assisted therapy has the potential to dramatically transform treatment for PTSD and should be expeditiously evaluated for clinical use.
PTSD is a common and debilitating condition that affects the lives of hundreds of millions of people annually. Once believed to be only tied to war experiences, there are actually a number of environmental and biological risk factors that contribute to the development and maintenance of PTSD.
PTSD can affect anyone and is typically comorbid with conditions that include childhood trauma, alcohol and substance use disorders, depression, suicidal ideation, and dissociation. In the study, MDMA was equally effective in participants with these types of comorbidities that are often associated with treatment resistance. Participants with the dissociative subtype of PTSD who received MDMA-assisted therapy had significant symptom reduction.
Dissociation
Dissociation is one of the most difficult aspects of treating PTSD.
It is a defensive mechanism where the person with PTSD blocks out their trauma because it’s too painful. This is especially common in childhood trauma where the incident happened decades ago and the person has either completely blocked it out, or changed details of it to make it seem less awful. It’s a useful technique in childhood, but maladaptive in adulthood.
Dissociation can also stall therapy, if the memory is too blocked out to be fully remembered it will be difficult to describe with clarity, and thus work out. The clearer these bad memories are, the more material the therapist and patient has to work with, and the patient can begin to understand why they are in a constant state of fear, even in a safe environment.
The tough part about a defense mechanism like dissociation works for a period of time. A child going through abuse might actually benefit from trying to forget what happened if they don’t have access to a therapist or even a family member they can trust.

The traumatized person will then subconsciously re-create dangerous and harmful situations that somewhat mirror their past experiences.
This is what many people call self-sabotage. Really the person isn’t actively sabotaging their life, there are subconscious patterns at work happening below the surface that without therapy the patient can sometimes never recognize. This can lead to destructive and unhealthy relationships, work environments, and habits. Without treatment, over a prolonged period of time, these propensities begin to structure a person’s personality and surroundings.
MAPS sees the dissociation aspect as one of the most important outcomes of the study,
Given that this covariate was significant, it warrants further study. Furthermore, given that other treatments for PTSD are not consistently effective for those with the dissociative subtype, these data, if replicated, would indicate an important novel therapeutic niche for MDMA-assisted therapy for typically hard-to-treat populations.
It’s a painful process for the patient, but all the experts in the field in trauma including Dr. Peter Levin, Dr. Alice Miller, and Dr. Bessel VanderKolk agree that one needs to be able to express the trauma in order for the healing process to happen. Disassociation is a form of repressing, the dam will eventually cave in, and if someone isn’t in a therapeutic setting when that happens the consequences can be ugly. Decades of unprocessed rage can cause violence, and decades of unprocessed shame can produce suicide ideation. Part of what makes trauma therapy so difficult is that to the nervous system, revisiting these memories feels the same as when they first happened.
The true opposite of depression is neither gaiety nor absence of pain, but vitality—the freedom to experience spontaneous feelings. It is part of the kaleidoscope of life that these feelings are not only happy, beautiful, or good but can reflect the entire range of human experience, including envy, jealousy, rage, disgust, greed, despair, and grief. But this freedom cannot be achieved if its childhood roots are cut off. Our access to the true self is possible only when we no longer have to be afraid of the intense emotional world of early childhood. Once we have experienced and become familiar with this world, it is no longer strange and threatening. – Alice Miller, The Drama of the Gifted Child
For extreme cases of PTSD people can develop alexithymia where the person cannot describe their emotions or how they feel. There weren’t any cases noted in this study, but I could see future studies in the field addressing this.
Window of tolerance
If the person has the self-awareness to know they are making their life more difficult, but don’t understand why they keep doing it this can lead to obvious frustrations and maladaptive behavior. We have to understand why our fight or flight mechanism is being triggered to lessen its importance in the present moment.
MDMA, when combined with therapy, may produce a ‘window of tolerance,’ in which participants are able to revisit and process traumatic content without becoming overwhelmed or encumbered by hyperarousal and dissociative symptoms. MDMA-assisted therapy may facilitate recall of negative or threatening memories with greater self-compassion and less PTSD-related shame and anger, according to a 2014 study.
People with PTSD often understandably have trust issues, even in a safe environment like a therapist’s office. Trauma survivors will often feel safe in dangerous environments, and in danger in safe environments. This can add another difficult variable to building a bond with a therapist as this can apply to people as well, pushing the healthy away and pulling the unhealthy in.
Therapy is vital for PTSD survivors. Even with the usage of MDMA, the therapy aspect can’t be ignored, the John’s Hopkins psilocybin for nicotine study included CBT (cognitive behavioral therapy). Re-processing traumatic memories is the key to healing the past.
I think MDMA’s now proven ability for patients to be able to access and process dissociative aspects of their PTSD is the biggest breakthrough here.